|
| |
Growth Monitoring
Health Basics: A supplement to Issue no. 24 - March 1986
pdf
 version of
this Issue version of
this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-6 Growth Monitoring
A supplement to Dialogue on Diarrhoea Online
Issue 24 - March 1986
|
DDOnline Growth
Monitoring supplement to DD24  Page 1 2
Page 1 2
HEALTH UPDATE Growth Monitoring
|
This insert gives a brief
overview of practical considerations for growth monitoring: what to measure, how to
measure, and types of equipment available for measuring growth. For a discussion of growth
monitoring issues, please see the article by Dr David Nabarro in DD
23 and="dd24.htm#page4">page 4 of DD 24DD 24. WHY MEASURE GROWTH? For a relatively small expenditure per child, growth monitoring can greatly strengthen
preventive health programmes. Growth is the best general index of the health of an
individual child, and regular measurements of growth permit the early detection of
malnutrition, frequently associated with diarrhoea, and other illnesses, when remedial
action is relatively easy. Although acute signs of malnutrition are easily noted by health
workers, it is often too late, and always more expensive, to help the severely
malnourished child.
|
 |
For early detection of children with growth retardation and high risk of malnutrition
and mortality, health workers need special tools and training in growth monitoring. The
growth status of children is a measure of the health and well-being of the whole
community. (Birth weight is of particular significance in determining the nutritional
status of a community: low birth weight is a good indicator of subsequent illness and
death in children.) Key issues to consider when setting up a growth
monitoring programme:
- what equipment is required?
- who will use the equipment and where?
- what will be done with the results?
- what is the programme's objective?
Problems associated with growth monitoring programmes
include:
- lack of understanding on the part of health workers about the role of growth monitoring;
many existing training methods only look at teaching the skills of growth chart completion
or checking it for errors;
- lack of involvement of mothers in monitoring the growth and development of their
children;
- lack of commitment of senior health personnel to the monitoring of children's growth and
development;
- lack of planning and facilities when children with growth faltering are detected.
WHAT TO MEASURE Various body measurements are used to assess growth. Some are easier to use, more
accurate and more useful than others. Monitoring the growth of a child usually requires
taking the same measurements at regular intervals and seeing how they change. A single
measurement only indicates the child's size at that moment; it does not give any
information about whether a child's size or weight is increasing, staying the same, or
declining. Careful repeated measurements and comparisons with previous measurements are
necessary because most children will continue to grow a little, unless they are very ill,
and it is easy to mistake some growth for adequate growth. Growth measures are usually
compared to a reference population. Gathering data to establish a local reference
population is a major undertaking. Therefore, western standards are usually used for
comparison, such as Tanner and Boston, or more recently, those of the National Centre for
Health Statistics (NCHS). Weight-for-age To obtain weight-for-age, the weight of the child (in kgs) is compared with that of a
healthy normal child of the same age from a reference population. This is the basis of the
weight-for-age or Gomez classification of nutritional status. A child weighing less than
60 per cent of the reference weight-for-age is considered to be severely malnourished.
|
|
DDOnline Growth
Monitoring supplement to DD24 1 Page 2 3
Looking at the current weight of a child in isolation is not very
useful. Most methods of growth monitoring, including weight-for-age, use a chart on which
a child's weight is plotted at intervals, ideally monthly, from birth to five years of
age.
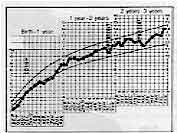 |
The child
whose growth is depicted on this chart made good progress, despite set-backs at the time
of coming off the breast and after a bout of measles. Weight loss was not allowed to
continue once it had been detected by the chart. Source: See How They Grow by David Morley and Margaret Woodland, Macmillan
Tropical Community Health Manual, 1979.
|
(Some programmes focus on children aged between 6 and 36 months, since this group is at
greatest risk from growth faltering - poor weight gain, or weight loss.) It is the
direction of the growth curve on the chart that is crucial, and a child whose growth curve
shows a levelling off or flattening needs help. A falling weight curve is a more urgent
sign for investigation and help. It is better to use weight-for-age in children aged 0 to
2 years than other anthropometric measures, because weight is a more sensitive indicator
during this period than height. Advantages of weight-for-age as a monitor of growth
- It is considered to be a useful indicator for growth monitoring in general terms.
- It is sensitive to small changes in the child's nutritional status, as reflected by
weight and is a good indicator for detecting growth faltering.
- The only tools needed are weighing scales and charts - usually easy to carry and
relatively cheap.
- Weighing is a fairly easy and quick task for inexperienced health workers although it
does require a health worker to be numerate.
Disadvantages
- Weighing should be done regularly and this is not always possible.
- It is necessary to know a child's age to the nearest month and this information is not
always available. (It is harder to estimate accurately the unknown ages of children over
two years old than those aged 0-2 years.)
- Mothers may object to their children being weighed by being suspended from hanging
scales, in some cultures, and many children feel frightened and insecure.
- Malnourished children - aged over one year - who have oedema or ascites may not be
classed as malnourished when in fact they are.
Weight-for-length / height This is a useful indicator where a child's age is unknown, or cannot be accurately
determined, or where it is not possible to weigh a child repeatedly over a period of time.
The degree of wasting can be assessed by comparing the child's weight with the weight that
would be expected for a healthy child of the same height.
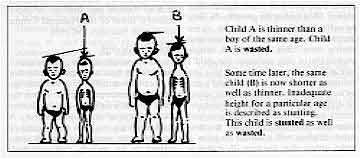 |
Child A is thinner than a boy of
the same age. Child A is wasted.
Some time later, the same child (B) is now shorter as well as thinner. Inadequate
height for a particular age is described as stunting. This child is stunted as well
as wasted.
|
To obtain weight-for-height, a child is weighed, its height measured and the weight of
the child being examined is divided by the weight of a reference child of the same height
to obtain a percentage. A child who is less than 70 per cent of the expected
weight-for-height is classed as severely wasted. (This cut-off-point is often used in
emergency situations to screen children to find who might benefit from special feeding
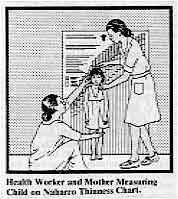
programmes.) The Nabarro chart, which does not involve the use of tables or calculations, consists
of a full-sized coloured chart which is mounted on a wall or a narrow chart mounted on a
12 cm wide plank.
|
Health Worker and Mother Measuring Child on Nabarro Thinness Chart.
Source: London School of Hygiene and Tropical Medicine, London,
U.K. The child is weighed and stood up against the chart opposite the bar representing his
weight. The position of the top of the child's head compared with the colour code of the
bar indicates if the child is wasted. (For a very young child it is better that the height
be measured lying down.)
|
 |
Advantages of weight-for-height as a monitor of growth
- It identifies the very thin or wasted child with definite malnutrition who requires
immediate attention.
- It is a good indicator to distinguish children who are well-proportioned from those who
are thin for their height. (Weight-for-age classifies many children as malnourished who
are short but have normal body proportions.)
- It does not require age data.
Disadvantages
- Stunted children with reasonable body proportions are classified as not malnourished,
but children who are short (stunted) and also thin, will be classified as wasted, rather
than stunted.
- Two pieces of equipment are required, a height as well as weighing scale. This adds to
expense and transportation problems.
- Taking two measures takes longer, and this is a problem for the busy health worker, more
training is also required and there is more chance of error.
- Some mothers may be reluctant to have their children weighed.
- Measuring height or length requires two people.
- It is more difficult for unskilled workers to learn to take accurate measurements of
length and height than to weigh a child.
|
|
DDOnline Growth
Monitoring supplement to DD24 2 Page 3 4
Height-for-age Height-for-age compares a child's height with the expected height for a healthy
reference child of the same age. The measure can be used to assess stunting, which may be
an index of long-term nutritional deprivation. A child who measures 85 per cent or less of
the standard reference height-for-age is considered to be severely stunted. Advantages of height-for-age as a monitor of growth
- It can indicate past nutritional problems and illnesses.
- A board for measuring length and height can be made locally at low cost and easily
transported.
- Mothers are rarely unhappy about a child being measured with a measuring board.
Disadvantages
- Changes in height occur relatively slowly compared with weight changes.
- It is not recommended as an independent measure.
- It is more difficult for unskilled workers to learn to take accurate measurements of
length and height than to weigh a child.
- Two people may be required to measure height/length and accurate age data are also
required.
Mid-upper arm circumference The circumference of the mid-upper arm (MUAC) increases in size during the first year
of a child's life quite significantly, but relatively little between the ages of one and
five years. At birth an infant's upper arm circumference is about 10.5 cms.
| By the age of one year it will
have grown on average to about 16.5 cms. Over the next four years until the child is five
years old, the circumference only grows about 1 cm to 17.5 cms at the most. Any child aged
between one and five years whose arm circumference is less than 12.5 cms may be
undernourished - and this cut-off point of 12.5 cms is most frequently used. Low MUAC is
more closely associated with acute malnutrition (wasting) than stunting. MUAC is useful as
a method of screening large numbers of children, during nutritional emergencies for
example, but it is less useful in longer-term growth monitoring programmes. |
 |
Advantages of MUAC as a monitor of growth
- A useful indicator of severe current malnutrition, whether or not stunting is present.
- It is quick to use and the measuring tape can be colour-coded for use by non-literate
health workers or the community.
- It does not require age data.
- There are no known objections by communities to this measure.
- Although MUAC does not indicate changes as rapidly as monitoring weight, it can be
useful to indicate changes in nutritional status.
- The arm tape is inexpensive and easily portable, and can be easily made by health
personnel.
Disadvantages
- It only identifies children with severe malnutrition, and it is not a sensitive early
predictor of malnutrition.
- There is a great variability in measurements. Finding the mid-point of the upper arm and
placing the tape around the arm without compressing the flesh is not easy.
HOW TO MEASURE Important criteria for choosing measuring equipment include:
- standardisation - consistent results using an instrument for a known measure;
- ability to maintain accuracy - reliability;
- ease of (correct) use, readability, portability;
- low cost, durability, ease of repair;
- local availability of equipment and cultural acceptability of the method.
Weighing scales In choosing scales the following criteria should be considered:
- The accuracy of the scale to nearest 250 gms (preferably the nearest 100 gms or quarter
of a pound, especially for young children).
- A total weight capacity of at least 25 kg, or 50 lbs., for programmes weighing children
under six (although the majority of critical weighings will be in children under 15 kg).
- Ease of reading numbers, with no confusion between kg and pound gradients if they are
both on the same scale. A direct transfer to growth charts and interpretation of the
results should be possible without mathematical calculations.
- Does not lift the baby too high off the ground/floor.
- An adjusting mechanism which allows the scale to be tared (this means to adjust the
needle to zero. If the needle rests on one side or other of zero the reading will be
inaccurate. When something like a basket to hold the child is hung on the scale this
weight needs to be subtracted before the child is weighed. If the scale can be tared it is
not necessary to subtract from the indicated weight).
- The reading point of the scale should be at eye level so that it can be read more
accurately.
|
|
DDOnline Growth
Monitoring supplement to DD24 3 Page 4 5
Scales can be locally manufactured,
but check accuracy by careful standardisation both during construction and during use.
Primitive scales may also be more difficult to use. Advantages include:
- less expensive;
- health workers gain new understanding and skills, if they and the community make the
scales;
- encourages self-reliance.
* A design for a locally made weighing scale, currently being field-tested, is
available from TALC. The scale requires a suitable spring and special weight charts, but,
it is hoped, it will involve mothers more closely in monitoring their children's growth. Commercially manufactured scales
are available in a variety of forms. Beam scales. Two types of single beam balance scales are used; both are
easily maintained and remain accurate over time.
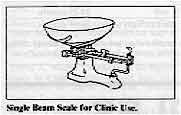 |
Single beam Scale for Clinic Use.
Source: CMS Weighing Equipment, Ltd., London, U.K. i) The model shown in the diagram is a floor or table type of scale in which the child
can sit or lie, and problems of having to suspend the child to weigh it are eliminated.
This variety has the disadvantages, however, of being hard to transport, and being more
expensive than most types of scales.
|
|
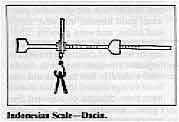
Indonesian Scale - Dacin.
Source: Nutrition Division, Ministry of Health, Jakarta, Indonesia. ii) The second type of beam scale is called a bar scale and has a free hanging beam. If
made from light materials this type of scale is easily transported. One general problem
with beam scales is that of keeping the child still.
|
 |
Spring hanging scales. These are usually spring scales which have either
a dial-face or are tubular.
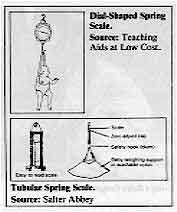 |
Dial-Shaped Spring Source: Teaching
Aids at Low Cost.
Tubular Spring Scale. Source: Salter Abbey i) Dial-faced scales are light, easily transportable, durable, fairly accurate and easy
to use. There have been problems with the internal parts of the scale rusting, and this
type of scale is one of the most expensive of the dial models.
ii) Tubular spring scales. These scales are light to transport, but are less durable
and more difficult to read than the dial-faced variety. The problem of reading the scale
is accentuated if the child is restless. The diagrams show a variety of methods of
suspending a child to weigh it. Considerations include the ages of the children to be
weighed and cultural acceptability.
|
In some places, for example, it may be better to use a net, hammock, box or basket,
rather than suspend the child in weighing pants. Bathroom-type scales. Although these are widely used, they are not
accurate, and become unreliable but they are portable and cheap. Digital scales. These electronic scales, a recent development, although
quick and easy to use, are still relatively expensive. The scale displays the exact weight
so that the health worker does not need to read the number from a continuous scale. Equipment for measuring arm circumference Measuring tapes should be made from durable, shrink-resistant material.
Suggested materials for home-made tapes include strong card, plastic-coated cloth, and old
X-ray film. Each measuring tape, whether commercially manufactured or produced locally
should be checked regularly against a standard ruler. The beginning of the tape should be
marked clearly on the arm measuring bands. There are several designs from simple strips to
slotted versions with sliding scales for interpretation at different ages. If the
"zero" is at the lead end of the tape, it avoids confusion but makes measuring
more difficult. The band can be marked in cms or colour coded in risk zones.
|
Keeping records The choice of record keeping system is important because the purpose of growth
monitoring can be achieved only when repeated measurements can be compared at intervals.
This is more useful than comparison with a reference population. The most useful type of
record-keeping system is that which requires the least mathematical calculation by the
health worker or mother and which shows whether the child is growing at an acceptable
rate.
- An important purpose of growth monitoring is to help the health worker assess the health
status of the individual child in order to decide on appropriate action, and to interest
the family in the health of the child.
- Another purpose is as a reminder to health workers about different aspects of child care
which should be reviewed.
- Another possible role for growth monitoring is to motivate and educate families.
Frequently, the cards are only designed for the record-keepers and not for teaching
mothers or other family members. Cards often provide no space to record the action
recommended to help the child. This could be a reminder for parents and health workers and
a focus for future discussion.
Considerations in chart design
- Size of the chart and the writing space. Size should be determined by the amount of
information to be recorded. There should be enough space to see changes in weight and
write in comments about diseases, advice given etc.
- Cultural context, The cultural beliefs and understanding of mothers should be
incorporated into the design to make the educational task easier. Cards for use by parents
should be in the local language with appropriate symbols.
- Ease of interpretation. Over-crowding with information and unnecessary lines only
confuses. Use only cut-off lines which are absolutely necessary to determine the
appropriate action for the child. Although different systems may be necessary because of
varying programme objectives, one type of card should be used in a single clinic or
village and preferably throughout the country.
|
|
DDOnline Growth
Monitoring supplement to DD24 4 Page 5 6
Equipment for measuring height and
length Two types of equipment are needed, for measuring standing height, and length lying
down.
|
Using a Baby Length Measuring Board. A well-designed measuring board can be used for both but may not be very portable.
Boards can be purchased or made locally.
|
 |
The weight-for-height, or 'thinness' chart, (Nabarro chart), contains a
height scale. It was described earlier, is easily transportable, light, measures
approximately 140 cms x 100 cms but is only made of thick paper. It is nailed or taped to
the wall so that the bottom of the chart is at ground level. Life size cutouts are
available for training purposes. Estimating a child's age Where a child's age is unknown the table shows some methods that may be useful in
estimating the child's approximate age. A local events calendar which includes harvest
time, religious festivals, or natural disasters, is most valuable. Also useful, is
comparing the child with other children in the village whose ages are known.
| The child is like this: |
So he is this old: |
| No teeth, can't sit alone
|
0-5 months |
| Has 1-6 teeth, can sit alone, can't walk alone
|
6-11 months |
| Has 6-18 teeth, can walk, knows a few words
|
12-23 months |
| Has 18-20 teeth, walks well, starting to talk well
|
24-35 months |
| Walks and runs well, talks well, has not yet lost first baby teeth |
36-59 months |
| Be careful: You should never look at the size of a child when
you are guessing his age. If the child is malnourished, his small size will make you think
he is younger than he really is. |
COUNTRY EXAMPLES Indonesia In Indonesia 2.5 million infants and young children are being weighed regularly at the
traditional monthly meetings of village women. The results are entered on growth charts
kept by the mothers themselves. Thailand In Thailand, a programme based on the home use of growth charts by parents in several
villages, helped to eliminate completely third degree malnutrition and reduce second
degree malnutrition by 44 per cent during 1981-1982, even though no additional food was
provided. Colombia In Colombia, improvements in weight gain for a majority of children suffering from
mild, moderate and severe malnutrition have been achieved in poor communities by nutrition
programmes incorporating the "Carnet de Salud" or health card kept at home by
mothers. Jamaica In Jamaica, a systematic programme to improve the health and growth of over 6,000 young
children using growth charts, immunisation and nutrition education and milk supplements,
has resulted in a 40 per cent decline in the prevalence of malnutrition and a 60 per cent
fall in infant mortality. Source: UNICEF State of the World's Children 1985. Ghana
- In Ghana a survey was undertaken to find out how mothers measured growth. Many cultures
have traditionally used a variety of indicators to measure their children's growth and
development. These should be taken into consideration and used by the community health
worker to understand the community's perceptions, so that they can be related to the use
of growth charts and mothers' participation be encouraged in improving child care.
Ghanaian mothers interviewed for the survey, believed that their children were growing
well when they: had a good appetite; were fat rather than thin; were learning new things
at the right time; seemed heavier when lifted; had normal bodily functions and healthy
skin and general appearance; good humour and were happy and active; and were growing
taller. Bead strings tied around the waist, legs or wrists of children were used as
indicators to measure growth. By the time a child is five months old, the bead strings
around the waist should have been changed or adjusted five times. Reasons given for poor
growth included: lack of food; insufficient breastmilk; a new pregnancy forcing the mother
to wean too early; bad feeding practices; not taking enough time to prepare food; and the
death of a parent. Growth and failure to grow were therefore associated with more than
just an increase or decrease in weight.
Source: Mothers and Children, Volume 5, Number 1. November-December 1985. American
Public Health Association.
|
|
DDOnline Growth
Monitoring supplement to DD24 5 Page 6
RESOURCE LIST BOOKS/MANUALS Cameron N. The Measurement of Human Growth. Available from Croom Helm Ltd.,
Provident House, Burrell Row, Beckenham, Kent, UK. 1984. Center for Disease Control and Health Service Administration. Weighing and Measuring
Children: A Training Manual for Supervisory Personnel. Atlanta, Georgia: Center for
Disease Control, 1980. Hendrata L. and Johnston M. Manual for Community Based Under-Fives Weighing
Programme. Indonesia: Yayasan Indonesia Sejahtera, 1978 Jelliffe D. B. Paediatrics in the Tropics. Available from TALC, 1985. Jelliffe D. B. The Assessment of the Nutritional Status of the Community. WHO.
1966. Morley D. and Woodland M. See How They Grow: Monitoring Child
Growth for Appropriate Health Care in Developing Countries. New
York: Oxford University Press, 1979. Tinibu A. Weight Charting and Its Significance in Child Health. Chapel Hill, NC:
University of North Carolina. African Health Training Institutions Project, 1978. Werner D. Helping Health Workers Learn: A Book of Methods, Aids and Ideas for
Instructions at the Village Level. Palo Alto: Hesperian Foundation, 1982. World Health Organization: Growth Charts and Home Based Child's Records in Maternal
and Child Health Care. An Appropriate Approach and Reference Manual for their
Evaluation. 1985. Available from WHO. World Health Organization Offset. Guidelines for Training Community Health Workers
in Nutrition. 2nd ed. 1986. Publication No. 59. ARTICLES Kielmann A. and McCord C. Weight-for-Age as an Index of Risk of Death in Children. Lancet,
1 (1978). p. 1247+ Nabarro D. and McNabb S. (1980), A Simple New Technique for Identifying Thin
Children. Journal of Tropical Medicine and Hygiene 83, 21-33. Seone N. and Latham M. Nutritional Anthropometry in the Identification of
Malnutrition in Childhood. Journal of Tropical Paediatrics and Environmental Child
Health, 17 (1971). p. 98 + SOURCES OF INFORMATION AND/OR EQUIPMENT Academy for Educational Development (AED), 1414 22nd Street, N. W., Washington D.C.
20037, U.S.A. Agency for International Development (AID), Office of Nutrition, Bureau of Science and
Technology, Agency for International Development, Washington D.C. 20523, U.S.A. American Public Health Association (APHA), Clearinghouse on Infant Feeding and Maternal
Nutrition, 1015 15th Street, NW., Washington D.C. 20005, U.S.A. AMREF, PO Box 30125, Nairobi, Kenya. CMS Weighing Equipment Ltd., 18 Camden High Street, London, NW1 0JH. U.K. Department of Human Nutrition, London School of Tropical Medicine and Hygiene, Keppel
Street, (Gower Street), London, WC1E 7HT, U. K. Departments of Tropical Paediatrics and International Community Health, Liverpool
School of Tropical Medicine, Pembroke Place, Liverpool, L3 5QA, U. K. Hesperian Foundation, 1919 Addison St., #304, Berkeley, CA 94704, U.S.A.
1-510-845-1447,="mailto:[email protected]">
[email protected] -
www.hesperian.org
Institute of Child Health, Tropical Child Health Unit, 30 Guilford Street, London, WC1,
U.K. National Center for Health Statistics, (NCHS), 3700 East-West Highway, Center Building
1-57, Hyattsville, MD 20782, U.S.A. OXFAM, Medical Unit, 274 Banbury Road, Oxford OX2 7DZ, U. K. Pan American Health Organization (PAHO), 525 23rd Street, N.W., Washington D.C. 20037,
U.S.A. Program for Appropriate Technology in Health (PATH), Canal Place, 130 Nickerson Street,
Seattle, Washington 98109, U. S. A. 98109, U.S.A. Salter Abbey, St Botolph's Lane, Bury-St Edmunds, Suffolk, U.K. Salter Industrial Measurement Limited, George Street, West Bromwich, West Midlands, B70
6AD, U.K. Save the Children Fund, (UK), 17 Grove Lane, London, SE5 8RD, U.K. Teaching Aids at Low Cost (TALC), PO Box 49, St. Albans, Herts AL1 4AX, U.K.* United Nations Children's Fund (UNICEF), United Nations, T-Plaza 4-1234C, New York, NY
10017, U.S.A. UNIPAC, UNICEF Procurement and Assembly Centre, UNICEF Plaus, Freeport - DK 2100,
Copenhagen O, Denmark. Voluntary Health Association of India (VHAI). C-14, Centre S.D.A., New Delhi 110016,
India. World Health Organization, Distribution and Sales Service, 1211 Geneva 27, Switzerland.
Cautionary note
It must be stressed that the practical benefits of growth monitoring in promoting
better nutritional status and child health are wholly dependent on effective follow-up
action being taken by mothers and health workers. This means that:
- mothers must be motivated and enabled to acquire the necessary skills and resources
to take action:
- any advice that is given to mothers must be culturally appropriate and compatible
with the resources that exist within the home and;
- basic health services must be readily available, including the provision of vaccines,
drugs and oral rehydration fluids.
Current experience suggests that growth monitoring programmes are not always
fulfilling these prerequisites and consequently are not achieving the desired impact on
child health. It is feared that this could lead to a backlash of disillusionment with
growth monitoring per se and it is therefore urged that growth monitoring should
not be instituted unless the proper infrastructure is in place to permit effective
follow-up action. Reference: Ashworth, A. and Feachem, R. G. Interventions for the control of
diarrhoeal diseases among young children: growth monitoring programmes. Document
CDD/86.
Geneva: World Health Organization, 1986.
ACKNOWLEDGEMENT
Much of the information contained in this insert is based on
material from the World Federation of Public Health Association's information for action
issue paper 'Growth Monitoring of Preschool Children: Practical Considerations for Primary
Health Care Projects.' 1985. Griffiths M. |
More detailed information concerning manufacturers of growth
monitoring equipment, costs, availability etc., is available from AHRTAG
|
Growth Monitoring
Health Basics: A supplement to Issue no. 24 March 1986
Page Navigation
This edition of Dialogue on Diarrhoea Online is
produced by Rehydration Project.
Dialogue on Diarrhoea was published four times a year in English,
Chinese, French, Portuguese, Spanish, Tamil, English/Urdu and Vietnamese and
reached more than a quarter of a million readers worldwide.
The
English edition of Dialogue on Diarrhoea was produced and distributed by
Healthlink
Worldwide.
Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any
uses made of the material.
|
updated: 23 August, 2019
|






