|
| |
Issue no. 13 - May 1983
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-8 Diarrhoea Dialogue Online Issue 13 -
May 1983
|
DDOnline
Diarrhoea Dialogue Online Issue 13 May
1983  Page 1 2
Page 1 2
Over to you...
Diarrhoea Dialogue promotes the
exchange of views and experiences among its readers. In this issue, we look particularly
at the progress being made around the world in oral rehydration therapy programmes. The
contributions from Tunisia, Peru and Egypt speak for themselves; as do the efforts of
UNICEF and WHO described on pages="#page4">four,="#page5">five and
six. W.A.M.C. and K.M.E. |
Tunisia: essentials for the future
Diarrhoeal disease is Tunisia's main health problem and, since 1980, WHO has been
assisting with the development of a national control programme. Before 1980, oral
rehydration using a simple sugar-salt solution was common practice in three regions of
Tunisia. However, this had little impact on the high national level of infant deaths due
to diarrhoea. Consultants Providing consultants is very helpful as they have a specific task to which they can
devote themselves. This is difficult for national staff involved with many other
activities, especially when they are responsible for planning and management. The objective of the first WHO mission was to discuss with the Tunisian authorities how
the programme would be set up and the role that WHO would play. The objectives of the second mission were to:
- Evaluate an awareness campaign carried out in 1980 on oral rehydration and the promotion
of oral rehydration salts.
- Plan a five year diarrhoeal disease control programme, even though specific objectives
had not been decided. We highly recommend use of the WHO document Manual for the
planning and evaluation of national diarrhoeal disease control programmes.
The third mission aimed to evaluate the implementation of the programme. Evaluation is
a delicate task for consultants. To find defects, they must be precise and objective. But
they must also be sensitive towards the workers interviewed. We recommend that consultants
sent to evaluate have the experience to be able to tell the difference between a minor
problem and a real obstacle to the development of a programme. The evaluation should provide an opportunity to find solutions to problems, not make
workers feel guilty. For national staff, diarrhoeal disease control work is yet another
task on top of their ordinary work load. For the best results, the programme should be
integrated with other activities. Supplies of ORS
|
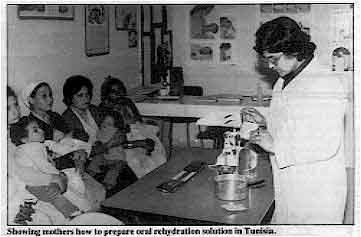
Showing mothers how to prepare oral rehydration solution in Tunisia. Apart from the Pharmacie Centrale de Tunisie (PCT), which provides Orasol (our brand
name for ORS) in small quantities, WHO and UNICEF have provided supplies of ORS. We would
like to take this opportunity to praise UNICEF's new interest in the problem of diarrhoea.
We recommend that they consider oral rehydration a priority and help in two ways in
particular:
|
 |
- Assisting research to solve some specific problems. For example: - to offer guidance about when the use of ORS is essential, so that demands for ORS do not
exceed the country's ability to manufacture and distribute it.
- to determine the ideal composition for ORS based on local biological and social factors.
- Encouraging wider distribution of ORS and promotion of oral rehydration. For promotion,
we suggest that ORS be considered as a medicine and could, therefore, benefit from the
involvement of pharmaceutical representatives. These could play a key role - especially
working with shops selling medicines, and with doctors.
Home-made solutions
We encourage the development of home-made solutions for prevention of dehydration.
These must be developed according to locally available resources and given at home as
soon as diarrhoea appears. The sugar-salt solution already in use here is acceptable
but should contain more calories. The taste should also be improved. Where available,
lemon is a useful addition as it adds potassium as well. Using the home-made solutions, ORS can then be kept for cases where the child does not
improve and has to be taken to a clinic or hospital. Logistic support
This consists essentially of training and health education materials funded by WHO.
Small equipment has been purchased locally while larger items have been purchased abroad
by WHO. Delays in delivery have occurred, as with supplies of ORS, which has slowed up the
implementation of the programme. When received, however, the materials caused great
interest. It became possible to hold a far greater number of training sessions at the
periphery and to spread them over the whole country. Audio visual support has maximised
their efficiency. Medical staff have been able to attend a number of awareness and training courses. For
example, regional workshops on diarrhoeal disease control, and a training course organized
by WHO-ICC for national CDD programme managers. At central level, information is well
disseminated through documents received regularly from WHO. Conclusion
In Tunisia, it was only in the 1970's that diarrhoeal disease was taken seriously
enough to begin a national control programme. We feel this was due in part to the very
strong influence of the medical education received in countries where diarrhoea is not a
problem, and more emphasis is put on 'modern medicine' than preventive and social
medicine. Where diarrhoea is still a major problem the WHO/CDD programme can play a key
role by spreading information about prevention and control. Dr S. Khadraoui, Co-ordinator of the Tunisian diarrhoeal diseases control programme,
and Dr B. Hamza, Director of the programme and of the National Institute for Child Health.
We express our thanks to WHO and UNICEF for their contributions to the Tunisian
programme and especially to Dr M. Merson, Director of the WHO Diarrhoeal Disease Control
Programme for his interest in the success of our programme. S. K and
B. H
|
In this issue...
- Reports from national programmes in Tunisia, Peru and Egypt
- WHO training courses
- UNICEF in action
|
|
DDOnline
Diarrhoea Dialogue Online Issue 13 May
1983 1 Page 2 3
Specific objectives
"So far, the relationships have been smooth and productive. This is due in
part to the personalities of the individuals involved and in part to the well-planned
nature of the campaign." Egypt has recently launched a national campaign to reduce childhood morbidity and
mortality due to diarrhoea. The campaign has various strategies including:
- the application of social marketing
- use of mass media
- clinical training of hundreds of practitioners at regional centres
- thorough study of the epidemiology and ethnography of diarrhoeal disease in different
areas of Egypt.
The national campaign comes under the Ministry of Health but has its own funding,
budget. steering committee and technical secretariat. One of its main functions is to
promote co-operation with many national, private voluntary and international agencies
dealing with diarrhoeal disease and nutrition. The campaign has become truly national
through joint research, support of services and teaching, and a national information
service (library, newsletter, "hotline", conferences and technical assistance). Agency support At the moment, the Egyptian campaign works with three international Agencies:
United States Agency for International Development (USAID), UNICEF and WHO. USAID is our
main external donor. UNICEF has supplied the Ministry of Health with start-up supplies of
Oralyte and given a production line to a state pharmaceutical company for producing
the salts in-country.
 |
Illustration
from a training set on preventing diarrhoea. We are also working with UNICEF in Egypt on several technical areas. WHO continues to
support training and research and is a generous supplier of information and ideas from
around the world. In turn, representatives from the Egyptian campaign acted as
facilitators on the recent regional mid-level course for CDD managers organized by WHO in
Alexandria
|
Productive So far, the relationships between all those involved have been smooth and productive.
This happy situation is due in part to individual personalities and in part to the
specific objectives of the campaign. If strains were to occur, they would probably develop
because of differences in methodology. However, since all aspects of the campaign will be
based on thorough, open testing and evaluation, we expect all dialogue to be creative and
mutually educative. Dr L. M. El-Sayyad, Executive Director, Diarrhoeal Disease Control Project, Egypt.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 13 May
1983 2 Page 3 4
'Salvadora': over-the-counter success
"Private manufacturers ... are well ahead of the primary health care planners
in promoting the use of ORT." In Peru, ORS has cut infant mortality rates remarkably. It is used at three levels of
medical care:
- in special intensive care units after initial intravenous treatment of severe
dehydration;
- as the treatment of choice for out-patient care in mild to moderate dehydration:
- to prevent dehydration appearing in any case of diarrhoea.
|
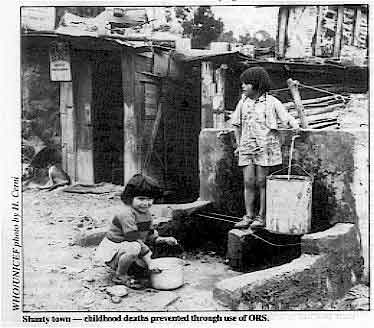
Shanty town - childhood deaths prevented through use of ORS.
As a result, in Lima and Trujillo, both crammed with shanty towns, during one summer
the number of infant deaths dropped by 50 per cent. This was due to a nationwide health
education campaign. ORS was advertised on television and radio in the same way as other
products. Thanks to this campaign, the ORS packets that in Peru are called Salvadora have
become one of the most widely used 'over-the-counter' medicines. The idea of the campaign
was to convince house-holders to have one or two packets of Salvadora at home to be
used as soon as diarrhoea affected any member of the family, especially children.
|
 |
Supply and logistics
One major problem is to have sufficient quantities of ORS packets and another is
logistics to ensure adequate distribution. Fortunately, the government of Peru is able to
manufacture ORS locally, through the state-owned LUSA laboratories. Management of
logistics relies on the not always efficient administrative structure of the Ministry of
Health. Agency response
It was impossible for Peru to seek assistance for the oral rehydration therapy campaign
from either bilateral or multilateral agencies for two main reasons:
- On political grounds, the government of Peru decided to handle the ORT programme on an
emergency basis. This was because of the shocking infant mortality rates due to diarrhoea
- 97 deaths per thousand live births. Under these circumstances, it was impossible for the
agencies to respond quickly enough. They need to go through very time-consuming planning
and bureaucratic procedures.
- The prevailing attitude towards project proposals in all agencies is that projects must
start in the agency itself and then go to the Ministries of Health. Where an idea has
originated within the government, the planning and implementation must nevertheless be
done the way the agency thinks best. There is a lack of confidence in the ability of
governments to manage a programme assisted by agencies. One safeguard might be for a
consortium of aid agencies to combine resources in support of national budgets for
specific projects.
Image of ORT As far as ORT is concerned, there is a need to improve its image among the general
population. The publicity techniques used by private companies for consumer goods must be
used for ORS. Latin America, and Peru especially, can reach almost all their populations
through radio and television. Generally speaking, the media are not being used by the
health services. Instead, emphasis is put on the so-called health promoters and field
workers to pass on messages. This gives another example of lack of confidence in the
capability of the general population to respond to mass media messages about primary
health care. Private manufacturers do not hold the same view and are well ahead of the
primary health care planners in promoting the use of ORT (as they have also been with
another important public health tool -soap!). The ideas expressed in this paper are to be used in countries like Peru that are not
regarded as being at extreme poverty level. Dr Uriel Garcia Caceres, Lima, Peru, former Minister of Health.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 13 May
1983 3 Page 4 5
| WHO training courses for diarrhoeal disease control |
Supervisory skills
Robert Hogan describes a new training course developed
by the WHO Diarrhoeal Diseases Control Programme (CDD) that is aimed at staff who
supervise a health facility and/or community health workers in developing countries. The skills taught on the course are not only of use in supervising the treatment and
control of diarrhoea but can also be used in other health services such as immunization
programmes, the treatment of acute respiratory infections, or malaria. The teaching method
is similar to that used on the training course for national programme managers developed
by CDD. This method stresses active participation by the students, allows them to work at
their own pace and gives frequent opportunities for them to practise what is being taught. The new supervisors course has already been field tested in Burma and will be further
tested in Jamaica and Egypt. Based on suggestions from staff and participants at these
field tests, a modified version of the course will be developed. It is expected that this
will be available in English by August 1, 1983 and in French and Spanish by October 1,
1983. Course materials The materials include an introduction and six modules. These are the main points
covered in each module: Community participation
- Work with the communities in your health area. Be sure the communities join in
discussions and help make decisions about health matters.
- Find out who has access to health services and who does not.
- Find out through discussion with the community what health problems are of greatest
concern to them.
- Discuss with community decision-makers possible ways of improving health services and
the health of the community.
- Reach agreement with the communities on how their resources and those of the Ministry of
Health will be used to improve health.
Treatment of diarrhoea
- Dehydration is the most important problem that must be treated in a patient with
diarrhoea.
- Families should be educated about proper treatment of diarrhoea in the home. This can
often prevent dehydration from occurring.
Health workers should:
- ask, look and feel for the signs of dehydration
- select a treatment plan based on the degree of dehydration
- check for signs and symptoms of serious problems other than diarrhoea and give treatment
where appropriate.
- A diarrhoea treatment wall-chart is included in this module to help health workers
remember how to assess and treat diarrhoea.
Targets
Targets help people to:
- know the goals they are working towards
- see their progress and feel proud of their work
- estimate what supplies and resources are needed.
- People will usually work harder to achieve targets if:
- the targets are realistic and
- they have helped to set the targets.
- To set realistic targets for usage of any health service, you first need to estimate
past usage of the service and consider ways to increase both access and usage.
Training
- Training should always include practice of tasks, in a situation as similar to
the job as possible.
- Before practising the task, learners should receive any necessary information and
examples.
- Different methods can be chosen to carry out training.
- Learners must receive feedback on their practice in order to know how well they
are doing a task and how they can improve.
- Evaluate training by watching learners working. If they still cannot carry out a task,
find out why. Use the results of evaluation to improve training.
Monitoring performance
- Monitoring the performance of health workers should help to discover any problems in
delivery of health services and help health workers improve their work. It should also
find work that is being done well.
- Before monitoring, decide what items are important to monitor, then decide how and when
to monitor each item. Checklists will help you remember what to look for.
- A rational, step-by-step approach should be used to find solutions to problems
identified in monitoring. Briefly, the steps are to:
- describe the problem;
- identify possible causes of each problem;
- find a reasonable solution to each problem;
- monitor the solution once it is implemented.
- After monitoring, always provide prompt feedback to health workers.
Monitoring and evaluating usage
- Monitoring usage of health services each month helps to find and correct problems
affecting usage of the services at an early stage.
- Evaluating whether usage targets for the year were achieved should indicate how much
progress has actually been made in increasing usage of health services, and increase the
accuracy of future usage targets.
- Monitoring and evaluating usage should also include trying to find out why usage
is up or down or why usage targets were or were not met, and taking appropriate
action. It is important to investigate reasons for both problems and successes.
Robert C. Hogan, Programme Management Officer, Diarrhoeal Diseases Control
Programme, World Health Organization, Geneva, Switzerland.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 13 May
1983 4 Page 5 6
| WHO training courses for diarrhoeal disease control |
Convincing the doctors
Accepting oral rehydration therapy can be hard for those accustomed to widespread
use of intravenous infusion. William Cutting reviews the courses
run by WHO to promote ORT to senior health staff. Education and training should not only transfer facts but also stimulate the
imagination. How successful are WHO's training courses in arousing the enthusiasm of local
doctors for the concept of oral rehydration?
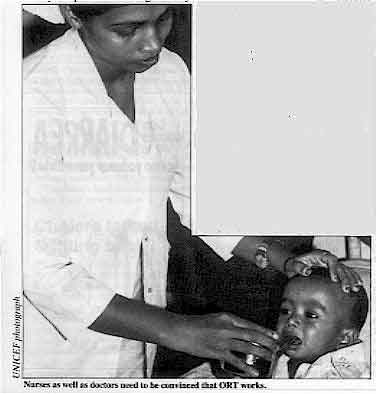 |
Nurses as well as doctors need to he convinced that ORT works. Many doctors have been accustomed to using intravenous infusions in the treatment of
diarrhoea and this can be lifesaving. They were also taught to 'rest the bowel' by
withholding food. Scientific studies may support the efficacy of oral rehydration but the
most convincing evidence is to be personally responsible for significantly dehydrated
patients and to watch them recover in response to an appropriate fluid given by mouth.
This has been the personal experience of numerous doctors who have attended training
programmes in different centres, but particularly in Dhaka, Bangladesh, at the
International Centre for Diarrhoeal Disease Research (ICDDR, B).
|
Learning by demonstration
The personal recommendation of a leading authority also carries great weight. Dr Dhiman
Barua, world expert on cholera and former director of WHO's diarrhoeal disease programme,
has taken a leading part in many of these training courses. Numerous doctors have
described how he walked up and down the diarrhoea wards for hours, spending time with each
trainee to reassure them and showing them how to give small amounts of ORS every few
minutes so that the amount of fluid going into the patient was more than the losses. Training huge numbers
Personal involvement and instruction by convinced teachers have been key elements in
many of the WHO-supported training schemes in recent years. Since 1979, regional and
inter-regional training centres have been operating in Bangladesh, India, Pakistan,
Indonesia and the Philippines. Fourteen countries in Asia and the Pacific region have
developed their own national plan for diarrhoeal disease control and most are running
their own national training programmes for health workers at different levels. The numbers to be trained are enormous, especially in countries like China and India.
Other nations have special problems of communication and supply - Indonesia and the
Philippines with their thousands of islands and Nepal with its rugged mountainous terrain.
It is in these situations that the new knowledge about the simple but effective oral
therapy for diarrhoea can be of critical value for isolated communities. Major impact already
Doctors have returned from regional and national training programmes and set up oral
rehydration centres. In one hospital in the Philippines, the result of opening such a
24-hour rehydration service was that over half the paediatric beds previously set aside
for diarrhoea patients could be re-allocated for other diseases. In another hospital,
following the training programmes and the emphasis on oral therapy, the cost of
rehydration fluids used in 1981 fell to less than half of the 1980 cost. Even in
established centres there was scope for improvements. At ICDDR, B, in the first half of
1980, only seven per cent of moderately severe dehydration cases were treated with oral
rehydration alone. By the same period in 1981, 61 per cent of similar cases were treated
exclusively by mouth. The courses have not only covered aspects of clinical management, but also the
managerial skills necessary to support CDD programmes at different levels. Training in
laboratory technology and epidemiology enables countries to monitor and evaluate their
national programmes and progress. For every training course a relevant curriculum has to
be developed, and written and visual material prepared. There is still a great need for
these to be adapted to the cultural context of the different peoples of many other
countries. There have been hundreds of courses and thousands of personnel trained, but in
many ways the task has just begun!
|
|
DDOnline
Diarrhoea Dialogue Online Issue 13 May
1983 5 Page 6 7
ORT in practice
"The need for ORT is clear. The technology is known. The means of
dissemination are available. The receptiveness of parents has been demonstrated. The cost
is small. And only an inexcusable lack of national and international will can now prevent
the bringing of its benefits to the vast majority of children in need."*
 |
Mother in Bangladesh giving oral rehydration solution to her children. The recent State of the World's Children Report 1982-83 published by UNICEF drew
international attention to the fact that some 15 million young children die every year
from a combination of malnutrition and disease and another five million from dehydration
caused by diarrhoeal diseases. The Report highlighted four main strategies that UNICEF is
strongly advocating which together could help to save the lives of 20,000 children per
day.
|
The four strategies are:
- Growth monitoring with charts
- Oral rehydration therapy
- Breastfeeding
- Immunization programmes
Of the four, ORT is perhaps the major strategy being advocated by UNICEF. Particular
emphasis will be put on the means of spreading information about ORT. As the Report
states: " . every available channel will have to be involved. The community's own
organizations, the radio and the mass media, the billboards and the adult education
centres, the women's groups and the community development workers, the primary health care
networks and the health services themselves."
|
These are examples of just some of the countries where UNICEF is heavily involved in
promotion of oral rehydration therapy: Nicaragua
|
Nicaraguan
leaflet about preventing diarrhoea.
- 300 oral rehydration units equipped serving over 155,000 children.
- 1,400 people trained to teach the use of oral rehydration salts, production of more than
a quarter of a million leaflets to explain the treatment to mothers.
- health volunteers (one for every 25 households) taught to carry the message about ORT,
and about preventive measures such as domestic hygiene and handwashing.
|
 |
Haiti
- a nationwide campaign to promote the use of ORT is underway backed by UNICEF and the Pan
American Health Organization (PAHO). The aim is to save the lives of 10,000 children a
year by 1987 - and to prevent the malnutrition of an even greater number
Bangladesh
- during 1982, half a million mothers taught how to prepare and use oral rehydration
salts. Follow-up surveys have shown that over 90 per cent of them are now able to make a
safe solution for their children.
India
- in Narangwal, the death of children aged between eight days and three years has already
been halved by community development workers using just oral rehydration salts and
penicillin.
|
* From the State of the World's Children Report 1982-83, published by UNICEF.
|
DDOnline
Diarrhoea Dialogue Online Issue 13 May
1983 6 Page 7 8
Required - sharp teeth and a strong wrist
Dr Mary Khalil Ibrahim, Dr Norbert Hirschhorn and Dr Loutfy M.
El-Sayyad, all working
on the National Control of Diarrhoeal Diseases Project in Egypt, have recently undertaken
a quantitative investigation of possible problems with various types of ORS packages
available in that country. The difficulties experienced by ten mothers, both in opening
the different packages and in dissolving the powders, were timed and observed. The mothers
were also asked to comment on their experiences with the packages.
|
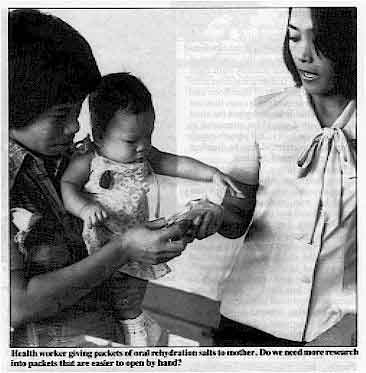
Health worker giving packets of oral rehydration salts to mother. Do we need
more research into packets that are easier to open by hand?
The investigation showed that ORS packed in a stiff paper envelope with an aluminium
liner inside was easier for mothers to handle than an aluminium foil packet, which
required teeth (or scissors) to open it, with the risk of spillage. The length of time
necessary to dissolve the powders varied and there were some differences between different
batches of the same product. All mothers favoured packages that were either easy to open
or quick to dissolve.
|
 |
It is suggested that packages that are difficult to open, or powders that are difficult
to dissolve, are likely to be barriers to initial or continued use of ORT. Research is
recommended into a safe form of packaging that is easy to open by hand. Standard
specifications for a powder that will dissolve easily need to be developed for use by any
company making a national ORS product. Comments from our readers on these aspects will be welcomed. Cholera tamed - or fighting back? Nearly ten years after it was replaced by the El Tor biotype of cholera, the
more virulent classical type of cholera bacterium suddenly reappeared in Bangladesh in
1982. It remains to be seen whether this finding is a local and temporary phenomenon or a
genuine change in the disease pattern. (1) Samadi et al 1983 Classical vibrio cholerae biotype displaces El Tor in
Bangladesh. The Lancet Vol. 1: 805- 807. King Faisal award The King Faisal International Prize in Medicine for 1984 will be awarded for specific
and original work in the field of diarrhoeal diseases. Nominations for the prize are
welcomed from research centres, universities and other educational institutions. The
closing date for receipt of published work is 20 August 1983. For full details write to:
Secretary General of the King Faisal International Prize, P. O. Box 22476: Riyadh 1195,
Kingdom of Saudi Arabia. Erratum
| Several readers have pointed out
the geographic error on="dd12.htm#page2">page two of Diarrhoea Dialogue 12
Diarrhoea Dialogue 12.The article on health education in schools in Dominica referred to the
Commonwealth of Dominica and not the Dominican Republic as stated. Our apologies to the
organizers of the seminars! |
 |
In the next issue...
We look at the use of 'social marketing' and mass media in the promotion of ORT
|
|
DDOnline
Diarrhoea Dialogue Online Issue 13 May
1983 7 Page 8
ORT for adults I find your Diarrhoea Dialogue very interesting and informative. We work with a
slum community on the outskirts of town and right on the seashore - some of the houses
actually built right over the water. Toilets are almost non-existent. We see lots of
diarrhoea and about 50 per cent of these cases turn out to be amoebic dysentery when the
stool is examined. I would be interested in any advice on how to kill amoebic cysts in
drinking water and how to disinfect babies' clothing and bedding. Recently a father became sick with severe diarrhoea, which turned out to be an amoebic
infection. When I saw him, he was very weak and felt nauseated and had drunk less than one
glass of water. I asked the mother why she hadn't come for some Orasol and she told me she
thought Orasol was only for the children. So we realized that we had to clarify our
teaching - everyone who gets diarrhoea needs to replace the lost fluids - children can
become dehydrated more quickly, but adults can also become seriously dehydrated. Anyway,
the father improved as soon as he got some Orasol and did not have to go to hospital. Diane E. Palmeri, RN, Family to Family, Inc, c/o Xavier University, Cagayan de Oro
City, Philippines.
Editors' note:
Amoebic cysts are killed if heated to 55°C. Drinking water needs thorough boiling.
Disinfecting clothing and bedding is not easy but it will help if it can be well boiled
and then dried in maximum sunlight. Education about personal and domestic hygiene is very important, especially about
food handling and the danger of flies which can act as cyst carriers. Rehydration is important in parasitic diarrhoea but it is also important, once the
cause has been identified, to give wherever possible the appropriate drugs to kill off the
parasites in the bowel and so cut down on the spread of infection.
No sugar available
|
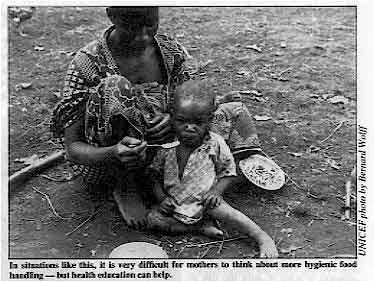
In situations like this, it is very difficult for mothers
to think about more hygienic food handling - but health education can help. I am working in a health clinic in Ghana as a nurse midwife, on a VSO project. Ghana
has many problems at the moment which affect our work but there is one in particular which
I feel someone at Diarrhoea Dialogue may be able to help me with. We have great
difficulty in obtaining sugar and the local people find it even harder. Thus we are having
a problem in teaching them how to make up oral rehydration fluid. The alternative I have
used so far is orange juice as it is plentiful, but I would be grateful for any
suggestions as to what else we may use to replace the sugar in our solution.
|
 |
Eleanor Hill, c/o VSO Field Office, P. O. Box 771, Accra, Ghana.
Editors' note: In an oral rehydration solution sugar may be replaced by a carbohydrate powder from
rice, and probably other cereals like maize. Either 30(1) or 50 gms (2) of flour from dry
or roasted rice has been found effective mixed with the other basic ingredients of ORS
(3.5gms salt, 1.5gms potassium chloride, 2.5gms of baking soda or sodium bicarbonate in
one litre of drinking water). (1 and 2). Orange juice supplies a little potassium and some
fruit sugar (fructose) which may also assist the absorption of sodium and water Perhaps the WHO and UNICEF representatives in Ghana can help you to obtain supplies
of ORS packets. (1) Molla et al 1982 Rice-powder electrolyte solution as oral therapy in diarrhoea
due to Vibrio cholerae and Escherichia coli. The Lancet Vol. 1: 1317-1319.
(2) Patra et al 1982 Is oral rice electrolyte solution superior to glucose
electrolyte solution in infantile diarrhoea? Archives of Disease in Childhood Vol. 57:
910-912.
|

Scientific editors Dr Katherine Elliott and Dr William Cutting
Executive editor Denise Ayres Editorial advisory group
Professor David Candy (UK)
Dr I Dogramaci (Turkey)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhorn (USA)
Dr D Mahalanabis (India)
Professor Leonardo Mata (Costa Rica)
Dr Mujibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Professor Andrew Tomkins (UK)
Dr Paul Vesin (France)
Dr M K Were (Kenya) With support from WHO, UNICEF GTZ and SIDA
|
Issue no. 13 May 1983
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 August, 2019
|






