|
| |
Epidemic Dysentery
Health Update: A supplement to Issue no. 55 - December 1993-February 1994
pdf
 version of
this Issue version of
this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-6 Epidemic dysentery
A supplement to Dialogue on Diarrhoea Online Issue 55
- December 1993-February 1994
|
DDOnline Epidemic
dysentery supplement to DD55  Page 1 2
Page 1 2
HEALTH UPDATE Epidemic dysentery Epidemics of bloody diarrhoea are currently sweeping through Africa, resulting in
the deaths of many adults and children. This DD supplement looks at what
causes epidemic dysentery and provides guidelines on preventing and managing epidemics.
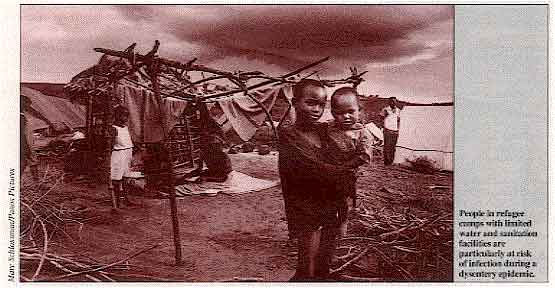
People in refugee camps with limited water and sanitation facilities are
particularly at risk of infection during a dysentery epidemic. Dysentery - bloody
diarrhoea - is one of the most dangerous types of diarrhoea. In general. it is more severe
and more likely to result in death than other forms of acute diarrhoea. Large scale outbreaks (epidemics) of dysentery are a particular threat to public
health. The death rate can be as high as 15 per cent, and health care services are
severely stretched during epidemics. Even when correctly treated, about 5 per cent of
people with dysentery can die during an epidemic. The bacterium responsible for epidemic dysentery is Shigella dysenteriae type 1
(Sd1 ) (1). S. dysenteriae is one of four species of Shigella.
The others are Shigella flexneri, Shigella sonnei and Shigella boydii. These
species are usually less dangerous than Sd1 and they do not cause large epidemics. Disease caused by Sd1 tends to be more common in infants, and elderly and malnourished
people. Mortality is also highest in these groups. Since Sd1 was first identified late last century, extensive epidemics have been
reported in Africa, Asia and Latin America. An epidemic of Sd1 in Latin America between
1969 and 1973 was responsible for more than 500,000 cases of dysentery and 20,000 deaths. Recently, a series of epidemics has been affecting countries in eastern, central and
southern Africa including Rwanda, Burundi, Malawi, Zambia, Zimbabwe, Swaziland and
Mozambique. There are no reliable data yet on the situation in Tanzania, Zaire and Angola,
but it is likely that Sd1 epidemics are also present in those countries. Political
upheaval in Burundi in October and November 1993 caused more than 650,000 people to flee
to neighbouring Tanzania and Rwanda, taking dysentery with them. Sd1 is one of the
main causes of death in refugee camps in countries who share a border with Burundi.
|
DEFINITIONS
- dysentery
bloody diarrhoea
- epidemic dysentery
large-scale outbreaks of bloody diarrhoea, almost always caused by Shigella dysenteriae
type 1 (Sd1)
- endemic dysentery
a normal incidence of bloody diarrhoea, caused by a range of organisms including Shigella.
- Shigella
a genus of bacteria with four species - Shigella dysenteriae, Shigella
flexneri, Shigella boydii and Shigella sonnei. Shigella causes the most
serious episodes of bloody diarrhoea
- shigellosis
infection caused by one of the Shigella species, often (but not always) associated
with bloody diarrhoea
|
|
DDOnline Epidemic
dysentery supplement to DD55 1 Page 23
Clinical features The main clinical sign of infection with Sd1 is bloody diarrhoea. Other symptoms can
include abdominal cramps, fever, or severe pain during defecation. However, bloody
diarrhoea during a dysentery epidemic is the only sign needed for diagnosing infection
with Sd1. Most cases are uncomplicated and self-limiting, lasting up to seven days. But dysentery
caused by Sd1 can also result in severe complications including persistent diarrhoea
(diarrhoea lasting 14 days or more), septicaemia (blood poisoning), rectal
prolapse, and
haemolytic-uraemic syndrome (HUS). HUS is a serious condition affecting the kidneys and
blood clotting system. Transmission Sd1 is extremely virulent - only a few bacteria need to be swallowed to cause illness.
As few as 10 -100 organisms can cause disease in adults. Because of this, Sd1 is
thought to be transmitted often through direct person to person contact. For example, a
person with faecally-contaminated hands can pass Sd1 bacteria to another person's hands.
The second person may swallow the germs and become ill with dysentery. (This is unlike
cholera which is mainly spread through contaminated food or water, and is rarely spread by
direct person to person contact.) Sd1 can also be transmitted through contaminated food
and water. Epidemics tend to occur during hot. humid and rainy seasons. although this is not
always the case. In epidemic areas, up to one-third of the population can be infected,
especially in crowded areas with inadequate sanitation, poor hygiene and limited supplies
of safe water. Other causes of dysentery While large-scale outbreaks of dysentery are almost always caused by Shigella
dysenteriae type 1, other types of bloody diarrhoea are often present
(endemic) in communities without reaching epidemic proportions. The most severe episodes of endemic dysentery are caused by other species of Shigella
- Shigella flexneri, Shigella boydii and Shigella sonnei.
Other pathogens causing endemic dysentery in children include: Campylobacter
jejuni, invasive strains of Escherichia coli, non-typhoid Salmonella strains
and Entamoeba histolytica. This DD supplement concentrates on Shigella dysenteriae type 1
because it is the cause of epidemic dysentery. Guidelines available soon WHO has recently revised its guidelines for the control of epidemics due to Shigella
dysenteriae type 1. WHO recognises that current knowledge regarding Sd1 is incomplete
and further research is needed. But much can be done to reduce the incidence and deaths
caused by Sd1. The guidelines describe the disease, its clinical features and
epidemiology. and
propose strategies for control and prevention. They provide the basis for the information
in this supplement, especially pages="#page3">3-4. The guidelines also explain steps health managers and workers faced with dysentery
epidemics can take to organise and use their resources effectively. The material for this supplement was written by Dr Ronald Waldman, CDR, WHO, CH-1211
Geneva 27, Switzerland with assistance from Dr Olivier Fontaine and Dr Leila Richards. 1. The cause of epidemic dysentery during the lost half of this
century has always been Shigella dysenteriae type 1 (Sd1) with one possible exception - an
outbreak of epidemic dysentery in Swaziland in 1992 where E. coli O157 was reported as the
cause; however Sd1 and Vibrio cholerae were also present in the population. The new WHO guidelines will be available in mid 1994. Write to: CDR, WHO, CH-1211
Geneva 27, Switzerland. For more information about treating endemic dysentery caused by Shigella, see the="su44.htm">shigellosis supplement in DD44.
|
A comparison of epidemics of dysentery and
cholera
|
| |
EPIDEMIC DYSENTERY |
CHOLERA |
| Causative organism |
Shigella dysenteriae type
1 |
Vibrio cholerae
O1 or
Vibrio cholerae O139 |
| Related organisms |
Other shigella species; C.
jejuni, certain E. coli, and E. histolytica can cause bloody
diarrhoea, but not epidemics |
Other V. cholerae
can cause profuse watery diarrhoea, but not epidemics |
Infective dose
(The number of organisms that need to be swallowed before a person becomes ill |
10 - 100 organisms |
1,000 - 1,000,000 organisms |
| Clinical features |
bloody diarrhoea, sometimes
with fever
abdominal cramps
pain on defecation |
profuse watery diarrhoea
dehydration |
| Complications |
persistent diarrhoea
septicaemia
rectal prolapse
haemolytic-uraemic syndrome |
severe dehydration leading
to shock (circulatory collapse)
electrolyte imbalance |
| Treatment |
antibiotics save lives
feeding is crucial
rehydration may be necessary |
rehydration saves lives
antibiotics shorten illness in severely ill patients |
| Antibiotics of choice
(according to sensitivity patterns) |
nalidixic acid
cotrimoxazole
ampicillin |
doxycycline
tetracycline
cotrimoxazole |
| Ages affected |
all |
all |
| Transmission |
person to person
food
water |
food
water |
| Attack rates |
up to 50 per 1,000
population |
1 - 20 per 1,000 population |
| Case-fatality rate in
untreated patients |
10 - 20% |
40% |
| Case-fatality rate in
treated patients |
about 5% |
less than 1% |
|
DDOnline Epidemic
dysentery supplement to DD55 2 Page 34
Detecting and managing an epidemic of Sd1
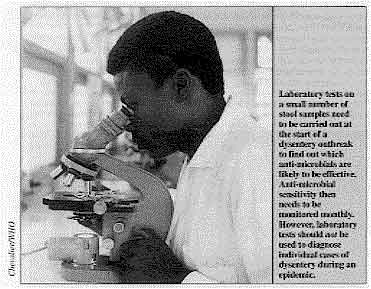 |
Laboratory tests on a small number of stool samples need to be
carried out at the start of a dysentery outbreak to find out which anti-microbials
are Iikely to be effective. Anti-microbial sensitivity then needs to be monitored monthly.
However, laboratory tests should not be used to diagnose individual cases of dysentery
during an epidemic. |
SURVEILLANCE Outbreaks of dysentery can only be detected early if a system for observing and
reporting disease has been established. This is called disease surveillance. A simple case record (showing the date, name, age and address of each patient; the
clinical diagnosis; and the treatment provided) should be kept at every health facility,
and information from case records should be reported regularly to the local health
authorities. This would ensure that outbreaks of epidemics were detected early. An epidemic should be suspected if there is a rapid increase in the daily or weekly
number of cases of bloody diarrhoea, or if increased deaths from bloody diarrhoea are
reported in a community. When an epidemic is suspected, health workers should immediately notify their
supervisors and request assistance from them. LABORATORY ANALYSIS When epidemic dysentery has been reported, all efforts should be made to confirm the
cause (which, in almost all cases, will be Shigella dysenteriae type 1) by
laboratory tests. The role of the laboratory during an epidemic of dysentery is two-fold: to confirm the
diagnosis and to establish which drugs the organism responds to. For these purposes, only a small number (e. g. 10-15 samples every 3-4 weeks) of stool
samples need to be collected, transported and tested. Special care needs to be taken in transporting stool samples containing S. dysenteriae
type 1 from outlying areas to central laboratories. This is because Sd1 organisms die
quickly if they are not stored correctly. Samples need to be kept in a special medium for
transportation and refrigerated. The guidelines available soon from WHO contain more
information about appropriate supplies and equipment for laboratories and how to transport
stool specimens. The laboratory should not be used to diagnose all cases of dysentery during an
epidemic. Once the organism causing the epidemic has been established, and an effective
anti-microbial to treat it identified, all cases of bloody diarrhoea should be treated
with that anti-microbial. PRIORITY TREATMENT The treatment for epidemic dysentery is anti-microbial drugs. Early treatment shortens
the duration of illness and reduces the risk of serious complications and death. Ideally,
all people with blood in their stools should be given anti-microbial treatment.
Unfortunately, during an epidemic effective drugs may not be available for all patients
with dysentery. It may be necessary to reserve treatment for those who are most likely to
die if they are not treated. Those most at risk are of dying from dysentery are:
- children less than two years old
- elderly people
- patients who are obviously malnourished
- patients with complications such as dehydration or fever
To avoid situations where treatment with drugs needs to be restricted, WHO will assist
national authorities to identify less expensive sources of effective drugs. CHOOSING AN EFFECTIVE ANTI-MICROBIAL Choosing the appropriate anti-microbial drug is not always easy. Over the last few
years. the organism causing epidemic dysentery -S. dysenteriae type 1 -
has become increasingly resistant to a variety of drugs. In some instances, only expensive
or less widely available drugs are effective. Wherever possible, laboratory tests should be done to find out which drugs Sd1 responds
to (called establishing anti-microbial sensitivity). Drugs to which Sd1 bacteria are
resistant in the laboratory should never be used to treat patients. Even if Sd1 responds
to a drug in a laboratory, the drug still needs to be assessed for clinical effectiveness
in patients.
|
|
DDOnline Epidemic
dysentery supplement to DD55 3 Page 45
The WHO guidelines suggest the following course of action:
- When laboratory confirmation or information about anti-microbial sensitivity is NOT
available, the anti-microbial drug of choice is currently nalidixic acid. It is
low-cost, has few side effects, and is widely available in most countries.
- When laboratory confirmation or information about anti-microbial sensitivity is
possible, three key anti-microbials - nalidixic acid, ampicillin and
trimethoprim-sulphamethoxazole (cotrimoxazole) - should be tested for sensitivity.
- When laboratory tests show that strains are resistant to nalidixic acid, ampicillin
and cotrimoxazole, other anti-microbials such as pivmecillinam (amdinocillin
pivoxil),
ciprofloxacin and norfloxacin are likely to be effective against Sd1. However, these drugs
are very expensive, so are not suitable for widespread use during an epidemic.
- Ineffective anti-microbials Sd1 has been consistently resistant to a wide variety
of other anti-microbials, including sulphonamides, streptomycin, tetracyclines and
chloramphenicol. These should not be used unless Sd1 has clearly been shown to be
sensitive to them.
A number of other drugs have never been shown to be effective in patients,
despite laboratory tests sometimes showing Sd1 bacteria are sensitive to them. These
include: furazolidone, gentamicin, and cephalosporins. When Sd1 is resistant to all available anti-microbials. cases of dysentery should be
managed with supportive therapy alone -oral rehydration and appropriate feeding (see="#page6">page 6). MONITORING IMPROVEMENT When a drug is effective, obvious improvement - increased appetite, decreased number of
stools, less blood in the stool, less fever, and less abdominal pain - normally occurs
within 48 hours. Patients who do not show signs of improvement 48 hours after the start of treatment
should be examined again. Treatment should change to an alternative anti-microbial to
which Sd1 is likely to respond. This is because laboratory tests of anti-microbial
sensitivity are not 100 per cent accurate. Failure of treatment does not mean that the
illness is caused by another organism, and drugs for other organisms such as amoebiasis
should not be given. LONGER TERM MEASURES After an epidemic has subsided, surveillance should continue to ensure that occasional
cases of shigellosis are promptly detected and treated. Efforts should be made to improve personal and domestic hygiene, water supplies and
sanitation facilities to try to prevent further epidemics (see prevention,="#page6">page 6). Preparations should be made for dealing with epidemics at both national and district
level. If further epidemics occur, control measures should be taken rapidly and
efficiently. Action to prepare for epidemics should include the following:
- supplies of oral rehydration salts, intravenous fluids and
anti-microbials should be
available at district and health facility level (see="#Clinic supplies">list of
supplies below)
- laboratories should be equipped and staff trained to identify the cause of dysentery and
to find out anti-microbial sensitivity patterns .
- health care workers should be trained in case management of epidemic dysentery.
The experience gained during the course of one epidemic of dysentery should be used to
strengthen the capacity of national diarrhoeal disease programmes to deal with all forms
of diarrhoea.
|
MAIN POINTS
- The case definition of dysentery is diarrhoea with visible blood in stools.
- A dysentery epidemic should be suspected if there is a rapid increase in the number of
cases, or deaths in a community from bloody diarrhoea.
- The cause of epidemic dysentery is almost always Shigella dysenteriae type 1.
- Anti-microbial treatment is required. Carry out laboratory tests on a small number of
stool samples to verify the cause of dysentery and establish what drugs the organism is
sensitive to. If testing is not possible, nalidixic acid is the anti-microbial of choice.
- All patients with dysentery should have their fluid intake increased and continue
feeding. Patients should be monitored for dehydration, and given oral rehydration therapy
if necessary.
|
Drug dosages for treating dysentery
caused by Sd1
|
| ANTI-MICROBIAL |
ADULTS |
CHILDREN |
| Ampicillin |
500mg
4 times daily for 5 days |
25mg/ kg
4 times daily for 5 days
(maximum 2g) |
Trimethoprim-
Sulphamethoxazole
(TMP/ SMX) |
TMP 160mg and
SMX 800mg*
2 times daily for 5 days |
TMP 5mg/ kg and
SMX 25mg/ kg 2 times daily for 5 days
(do not exceed the adult dose) |
| Nalidixic acid |
1g
4 times daily for 5 days |
55mg/ kg per day
Divide into 4 separate doses and give 4 times daily for 5 days
(maximum 4g) |
| *TMP/ SMX is a fixed-combination product: the ratio of TMP to
SMX is always 1:5.
|
Clinic
supplies for 100 persons with dysentery
|
| Treatment Supplies |
100 bars soap
30 boxes soap powder for washing clothes
2 bottles cleaning solution (2% chlorine or l-2% phenol) |
| Rehydration Supplies |
100 packets ORS (for 1 litre per patient)
10 litres Ringer's lactate solution
5 scalp vein sets |
| Anti-Microbials |
1600 x 1 gm tablets of nalidixic acid
Other anti-microbials may be needed instead of nalidixic acid, depending on local drug
sensitivity |
| Other Supplies |
1 large container for drinking water
5 x 1 litre bottles for mixing ORS solution
10 glasses for drinking
5 teaspoons |
|
DDOnline Epidemic
dysentery supplement to DD55 4 Page 56
Refugee crisis spreads disease
Studies in one of the African countries worst hit by the current epidemics -
Burundi - have indicated possible risk factors for becoming ill with dysentery. Over the last twelve years the east African
state of Burundi has experienced regular annual outbreaks of dysentery, peaking in the
rainy seasons (September to December). In 1992 and 1993 particularly severe epidemics swept across the country. In 1992,
almost 80,000 cases were reported - a national incidence of 14.2 cases per 1,000 people.
|
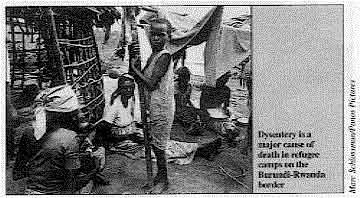
Dysentery is a major cause of death in refugee camps on
the Burundi-Rwanda border This year. a refugee crisis has increased the severity of the epidemic. As a result of
political and social upheaval, hundreds of thousands of Burundians have fled to
neighbouring Rwanda, Tanzania and Zaire, and spread the epidemic to refugee camps.
|
 |
WHO and the United Nations High Commission for Refugees are working with other relief
organisations to coordinate a response to the epidemic. Three studies in Burundi between 1990 and 1993 show that epidemic dysentery is a
serious problem with high mortality rates, and that a rapidly changing pattern of
sensitivity to drugs makes treatment difficult. In 1990, Ries et al. collected 189 stool samples from patients in Gitega province with
bloody diarrhoea. An organism causing dysentery was isolated in 125 samples. Of these, 66
per cent were Shigella dysenteriae type 1 (Sd1), and a further 25 per cent were
other Shigella species. Sd1 strains were resistant to nalidixic acid, ampicillin,
cotrimoxazole. tetracycline
and chloramphenicol. The only drugs Sd1 responded to - ciprofloxacin, pivmecillinam and
ceftriaxone - were expensive and were not available in large quantities at short notice. A community survey of 9,300 inhabitants in the same province was conducted by
Birmingham et al. in February to September 1992. The incidence of bloody diarrhoea during
the epidemic was found to be 13.9 per 1,000 people. Incidence increased with age. Possible
risk factors for becoming ill included: use of a cloth rag for anal cleansing following
defecation; recent loss of weight; and little or no schooling. In March 1993, Murray et al. followed up 775 patients who had reported to health
facilities in Muramvya province with bloody diarrhoea in the previous six months. Seven
per cent of patients (including many who had received treatment) had died. The median
interval between the onset of symptoms and death was 13 days. The researchers also collected 133 stool samples, 35 per cent of which yielded Sd1.
Significantly, the resistance pattern to drugs had changed.* While
Sd1 was still resistant to ampicillin and cotrimoxazole, it was now sensitive to nalidixic
acid, as well as the more expensive drugs found to be effective before -
ciprofloxacin,
pivmecillinam and ceftriaxone. This meant that nalidixic acid was the clear drug of
choice. The Burundi studies show that anti-microbial sensitivity patterns can change rapidly.
Therefore, active laboratory monitoring systems need to be established before the onset of
an epidemic. The studies also indicate that much more needs to be found out about risk
factors and transmission. Adapted from Manirankunda, L et al.. 1993. The epidemiology of bacillary dysentery
in Burundi. Bulletin Epidémiologique du Burundi, July-September. *Although the studies were done in different provinces, there is no
reason to suggest that sensitivity patterns would differ from province to province during
a nationwide epidemic. South Asia also affected by Sd1 During a south Asian epidemic in 1976, Shigella
dysenteriae type 1 spread from south India to Sri Lanka. Sd1 is now endemic in Sri
Lanka, with epidemics occurring periodically. Problems of civil unrest and migration of refugees from 1985-1992 led to a sharp
increase in cases of dysentery, with the number of cases more than tripling (from 79 cases
per 100,000 people, to 245 per 100,000) in this period. Lack of awareness about the way the disease spreads has been a major factor in epidemic
transmission. A study in the town of Galle showed that while more than 90 per cent of the
adult population used toilets, the stools of about 70 per cent of children were
disposed of outside, in open pits or simply left on exposed ground. The anti-microbial sensitivity pattern has changed considerably between epidemics. In
the first epidemic between 1976 and 1978, Sd1 was sensitive to nalidixic acid. During the
next epidemic (1978-9) Sd1 continued to respond to nalidixic acid. However, between 1982
and 1989, Sd1 was found to be resistant to nalidixic acid, but was sensitive to other
drugs at various times, including pivmecillinam. Professor D G Harendra de Silva, Professor of Paediatrics, Faculty of Medicine,
University of Ruhuna, Karapitiya, Galle, Sri Lanka.
|
|
DDOnline Epidemic
dysentery supplement to DD55 5 Page 6
Supportive treatment is vital
In addition to life-saving anti-microbial treatment, all patients with dysentery
caused by Sd1 need to drink more and to continue normal feeding. INCREASING FLUIDS It is crucial for people with dysentery to drink more liquids (including plain water)
in order to prevent dehydration. Readily available home fluids (such as yoghurt drinks; water in which a cereal has been
cooked; unsweetened tea; green coconut water; and fresh, unsweetened fruit juice) are good
choices. If possible, dysentery patients should also be given a fluid that contains salt,
e. g. salted soup, salted rice fluid or oral rehydration fluid. Patients with dysentery should be assessed regularly for signs of dehydration. The key
signs are: increased thirst; restlessness; irritability; and loss of skin elasticity (when
the skin is pinched and released it does not flatten immediately). If dehydration becomes
severe, a patient may become lethargic or unconscious and be unable to drink. If the patient shows signs of dehydration, they should be given rehydration fluid
immediately. There are three main types of rehydration fluid: oral rehydration salts (ORS)
solution, sugar-salt solution (SSS) and cereal-based solutions. Oral rehydration fluid
should be given at a steady rate in small amounts. Children under two years old should
receive at least l/4 - 1/2 cup of rehydration fluid after each loose stool. Older children
should receive at least 1/2 - 1 cup. Children over 10 years old should drink as much
rehydration fluid as they want. For more information about oral rehydration therapy, see="dd52.htm">DD52. CONTINUING FEEDING Continuing to give nutritious food to people with dysentery is very important. A major
complication of dysentery is weight loss and rapid worsening of nutritional status. This
is because people with dysentery often have reduced appetites, yet their bodies need more
nutrients than usual in order to fight infection, repair tissue damage, and replace
nutrients lost during diarrhoea.
|
Eating well can ensure a good recovery after a dysentery attack.
Even when patients survive dysentery, resultant malnutrition may increase their
vulnerability to other life-threatening illnesses. In general, the same foods should be given during dysentery as those a patient eats
when he or she is well. Meals may need to be given in smaller amounts more frequently. and
carers should gently but persistently encourage people with dysentery to eat. If possible,
food rich in potassium such as spinach, avocado pears, bananas and coconut water should be
given. Even if patients are well fed, they may have lost weight and be malnourished after the
dysentery episode is over. Providing an extra meal every day for two weeks can help to
restore lost weight.
|
 |
If infants with dysentery are normally breastfed, mothers should continue to breastfeed
them frequently. If infants under four months old normally receive other foods in addition
to breastmilk, these should also be continued during an episode of dysentery and mothers
encouraged to breastfeed frequently. However, after the dysentery episode health workers
should find time to encourage these mothers to practise exclusive breastfeeding until
their infants are at least four months old. For more information about feeding during diarrhoea, including when diarrhoea lasts
14 days or more, see="dd53.htm">DD53. Prevention strategies Like other forms of
diarrhoea, Sd1 infection is spread through human faeces. When people become infected with
Sd1, they excrete large numbers of Sd1 organisms in their stools. If germs from these
stools come into contact with food or water, other people can swallow them and become
infected. In addition, Sd1 bacteria are so infectious that sufficient organisms to cause
disease can be spread from one person's hands to another's The only proven ways of preventing infection and transmission of all forms of Shigella
are handwashing with soap and breastfeeding. Methods for preventing other forms of
diarrhoea are also likely to reduce transmission of Sd1, although there is no research
showing this. These methods include: the promotion of commercial and household food
hygiene; the provision of adequate supplies of clean water for drinking; and the safe
disposal of human faeces. Handwashing Thorough handwashing with soap appears to be the single most effective way to prevent
transmission of all forms of Shigella. The key times for handwashing are: after
defecation; after cleaning a child who has defecated or after disposing of their stools;
and before preparing or eating food. Health care workers should wash their hands before
and after examining each patient and before giving ORS or food to a patient. It is now known that people are more likely to wash their hands if they have easy
access to a plentiful supply of water. Water for washing and drinking should be stored in
different containers. If soap is not available, ash or mud can be used. If possible, in areas affected by
dysentery epidemics, soap should be distributed to families who cannot afford it. After handwashing, hands should be dried with a clean cloth or left to dry naturally in
the air. Hands should not be dried with a dirty cloth. Breastfeeding Breastfed infants are much less likely to get dysentery than other infants. If
breastfed infants do get dysentery, their illness is likely to be much milder than in
infants who are not breastfed. For more information about prevention, see DDs="dd54.htm">54,="dd45.htm">45 and="dd44.htm">44.
|
Epidemic dysentery
Health Update - A supplement to Issue no. 55
December 1993 - February 1994
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 August, 2019
|






