|
| |
Issue no. 2 - August 1980
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-8 - Diarrhoea Dialogue Online Issue 2 - August
1980
|
DDOnline
Diarrhoea Dialogue Online Issue 2 August 1980 . Page 1 2
Page 1 2
BREAST OR BOTTLE
We were delighted that so many readers commented on the tin of baby milk powder in the
picture from the Philippines on="dd01.htm#page7">page seven of the first issue
of Diarrhoea Dialogue. Everyone needs to be very much aware of the dangers involved
when bottle-feeding becomes fashionable in parts of the world where the milk powder will
inevitably be mixed with unsafe water in an unclean bottle, in insufficient amounts.
Poverty and ignorance are to blame, not the mothers, if bottle-feeding replaces
breastfeeding and the feeding bottle becomes the baby-killer through diarrhoeal disease
and malnutrition.
 |
Better health education on infant feeding.
WHO photo by J. Abcede. Diarrhoea Dialogue is well aware of the many sides to the baby food controversy;
later issues will highlight some of these. Meanwhile it is good to see that the 33rd World
Health Assembly in May endorsed the recommendations from the WHO/UNICEF meeting on infant
and young child feeding, held in October of last year. (1) These ask for promotion of
breastfeeding; work on the development of weaning foods based on local products; better
health education, training and information on infant feeding; and the preparation of an
international code of marketing practice. The International Baby Food Action Network is
acting as a watchdog meanwhile to discourage milk power advertising which influences
mothers not to breastfeed their babies.
|
Obviously there is still a long way to go but the way is becoming more clearly
signposted. Papua New Guinea seems to have got off to a flying start by making feeding
bottles available only on prescription.(2) We hope to hear what is happening in other
countries to help meet the WHO/UNICEF recommendations. 1 Code of marketing practice 1980. The Lancet vol 1: 1239-1240
WHO/ UNICEF 1979 Joint WHO/UNICEF meeting on infant and young child feeding. WHO, 1211
Geneva 27, Switzerland 2 Aidou J et al 1979 Bottle-feeding and the law in Papua New Guinea. The Lancet vol
1: 155 Who reads Diarrhoea Dialogue
The first and most important group we aim to reach are the primary health care workers
- those who are actually caring for children with diarrhoea. Within this group, there will
be people with little or no knowledge of English. We hope that their trainers will help
here by passing on the information in the newsletter and translating useful articles (see
note on="#page2">page two). Secondly, we are aiming at health planners and administrators who need to know about
the dimensions and nature of the diarrhoea problem, so that they can apply their
management skills to combat it. The third group are scientists and research workers who require information about new
methods and techniques being tried out in other parts of the world, but may not have the
opportunity of seeing all the relevant journals and papers. Finally, we hope to reach all those who have a general interest in health matters. In
each issue of the newsletter we intend to have items that will be of interest to all these
groups. If you feel that the balance is wrong, let us have your views. Response to the="dd01.htm">first issue of Diarrhoea Dialogue has shown that the newsletter
is reaching all of its target groups. Many of you have written to us already to give your
views on the content, design and future development of the publication. We have been
delighted and encouraged by your response and the evidence that the newsletter will serve
a real need. W.A.M.C. and K.M.E.
|
In this issue . . .
- Jon Rohde discusses the importance of drinking in diarrhoea
- what are the signs of dehydration?
- news from Bangladesh, Turkey and The Gambia
- questions and answers
|
|
DDOnline
Diarrhoea Dialogue Online Issue 2 August 1980 . 1 Page 2 3
Oral rehydration bibliography
 |
This is a
very valuable review, which summarises 133 publications dealing with oral therapy of
diarrhoea. The contents are set out in chronological order under five different headings:
history, clinical trials, composition, impact and implementation. Each paper, study or
letter is reviewed, often with a short comment on the relevance of the authors'
conclusions. Some articles naturally cover several topics and there is adequate
cross-referencing. |
It provides important reference text for field and research workers concerned with
diarrhoeal disease. Could it be improved in any way? It contains indexes by author and
country, but not by subject. An alternative to a subject index might be to break down the
five major titles into sub-titles for the main areas covered.
Even with the concerted efforts of individuals and organisations all over the world,
diarrhoeal disease and its serious consequences are likely to be a problem for many years.
Readers of Diarrhoea Dialogue have already been asking for an annotated
bibliography about diarrhoeal disease. This publication meets that need and will be of
practical value well into the future. However, because knowledge about prevention and
management of diarrhoea is constantly increasing, the bibliography will need to be revised
and updated every year or two. It is good to know there are plans to do this. Free copies
of the bibliography are available from PAHO, 525, Twenty-third Street, N. W., Washington
D.C., 20037, U.S.A.
Baumslag Net al 1980 Oral rehydration therapy: an annotated bibliography. Pan
American Health Organization. pp 112, Spanish and English, free. ORT in Turkey Several interesting results emerged from an oral rehydration therapy (ORT) field study
carried out in Ankara last year. Auxiliary nurse midwives were assigned to give ORT at
home and to teach mothers to use the fluid. The ingredients were provided pre-packaged,
mostly by UNICEF. The study was preceded by an information drive to educate the mothers on
the need for early administration of the rehydration fluid and the importance of feeding a
child suffering from diarrhoea. The mothers' acceptance of ORT was high. It was found that consumption of the oral
fluid increased when its taste was good. Some of the locally made mixtures were not found
to be as palatable as the one supplied by UNICEF, and this was reflected in the acceptance
of fluid by the children. Another interesting observation was the clear preferences of the
mothers to use ready-made packages rather than the "pinch and scoop" method. In the Turkish experience, the use of ORT can be increased by:
- participation of the community in the programme
- provision of the ingredients in packages carrying health education messages to the mothers
- distribution of the packages through grocers' stores, in addition to the health services, to ensure availability
- inclusion of ORT in the curriculum of medical students and adopting this method of treatment in hospitals.
Bertan M., Egeman A. 1979 ORT: the Turkish experience. WHO Chronicle vol 33: 132.
Infant foods and weanling diarrhoea
 |
Contamination of infant foods may be a
casual factor in weanling diarrhoea.
WHO photo by J. Mohr In rural areas of The Gambia where there may be a shortage of firewood, it is common
practice to prepare enough infant foods to last all day rather than for one meal. The food
frequently becomes contaminated, especially during the rainy season. This contamination
may be a casual factor in weanling diarrhoea.
|
Members of the United Kingdom Medical Research Council Dunn Nutrition Unit carried out
a study in Keneba, a subsistence farming community in The Gambia. They discovered that a
high proportion of food consumed by infants and young children was overgrown with
bacteria. More thorough cooking methods failed to prevent contamination, the most
effective solution being to eat the food as soon as possible after preparation. Unfortunately, the conveniently thin gruels given to infants when breastfeeding has
stopped are not only poor nutritionally but also easily contaminated. During the rainy
season when diarrhoeal illness is at a peak, levels of food and water contamination are
also greatest. The seasonal nature of intensive farming also results in a lowering of the
standards of child care at this time. Barrell R. A. E., Rowland M. G. M. 1979 Infant foods as a potential source of
diarrhoeal illness in rural West Africa. Transactions of the Royal Society of Tropical
Medicine and Hygiene vol 73 (1): 85-90. Reproduction and translation
We are happy for readers to translate and reproduce articles or abstracts from Diarrhoea
Dialogue in their own publications with a suitable acknowledgement to
AHRTAG. Please
send us a copy! Many of you have written to ask whether the newsletter will be published
in other languages in the future. Translation into French, Spanish, Portuguese and Arabic
is being planned and we will keep you informed about availability.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 2 August 1980 . 2 Page 3 4
Stickiness and sickness A symposium held at the Ciba Foundation in May discussed the relationship between the
adhesion of micro-organisms and disease. Several participants illustrated how this area of
scientific research has particular relevance for the mechanisms and control of some
diarrhoeas. Bacteria such as Escherichia coli can stick to the gut lining by means
of hair-like structures called 'pili' or 'fimbriae' which enable them to colonise and
cause diarrhoea. Bacteria that don't stick are expelled without causing any symptoms in
the host. Veterinary scientists have already discovered that strains of E. coli that
were causing diarrhoea in piglets were not virulent unless they possessed pili called K88.
A vaccine based on K88 has now been developed that protects by preventing the adhesion of E.
coli to the intestine of piglets. The mother pig is vaccinated and her milk contains
the protective anti-body against K88. Dr M. M. Levine and his colleagues at Maryland University, Baltimore are looking at
strains of E. coli that cause infant and travellers' diarrhoea. There are
antigenically distinct types of pili and scientists must aim to make a vaccine that
stimulates the body's defence against sufficient of them to give wide protection from
virulent strains. The Maryland team are looking for the most suitable combination to test
as a basis for a vaccine. Dr Levine thinks that it will need to consist of about five
sorts of pili. Ciba Foundation 1981 Adhesion and microorganism pathogenicity (Ciba Foundation
Symposium 80). Pitman Medical, Tunbridge Wells. Soap, water and shigellosis
Approximately six per cent of Dacca's population is affected by shigellosis and the
incidence is increasing steadily. Shigellosis is an infection of the large intestine by a
group of bacteria which frequently cause dysentery; diarrhoea with blood, pus and mucus in
the stools. It is an acute condition coming on suddenly and is usually accompanied by
fever, vomiting and abdominal pain. The rate of secondary infection ranges from 20-25 per
cent. In hospitalized cases, the mortality rates for severe shigellosis have been from 10
to 15 times higher than for cholera - indicating that simple rehydration is inadequate for
treating this bacillus. The use of vaccines has not been encouraging and resistance to
multiple antibiotics is increasing.
 |
The whole situation is compounded by the appalling lack of sanitation in Dacca. Members of the International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR, B) decided to find out whether a simple intervention, without other changes in the environment or community, might lower the rate of shigellosis. Hand washing with soap and water was chosen as a possibility. |
On the basis of stool cultures, cases and controls were selected from the hospital for
a ten day follow up. Age, socio-economic status and neighbourhoods were matched in
selecting controls. Two to three pieces of soap and earthenware pitchers for carrying
water were supplied to the study families. People were advised to wash their hands with
soap and water before meals. Regular checks were made to see whether or not the soap was
being used.
|
Handwashing - a simple but effective practice to encourage.
WHO photo by D. Henrioud The overall secondary infection rate in the hand-washing group was 10.4 per cent and in
the control group 32.4 per cent. The secondary case rate in the hand-washing group was 2.2
per cent and in the control group 14.2 per cent. Providing soap and water considerably
reduced both the secondary infection rate and the severe effects of the disease. It seems
that a simple intervention such as this, easily understood and implemented even in adverse
surroundings, can be very beneficial.
|
 |
(Personal communication from Dr M. U. Khan) CHILD-to-child
A programme is being run at the Institute of Child Health in London promoting ways in
which children can contribute to the healthy development of younger brothers and sisters.
For example, older children can give oral rehydration to younger members of the family
with diarrhoea. Do you know of any cases where this is happening? The Institute of Child
Health is offering a prize of books to anyone whose true account of older children helping
to rehydrate younger children is published in Diarrhoea Dialogue. Please send your
letters to the Executive Editor, Diarrhoea Dialogue, AHRTAG, 85 Marylebone High
Street, London W1M 3DE, England.
The next issue...
- is planned for November/December 1980
- will contain a main feature on health education in relation to diarrhoea
- will report on a diarrhoeal diseases control training programme for national programme managers being organized by WHO
- will continue our practical advice series
|
|
|
DDOnline
Diarrhoea Dialogue Online Issue 2 August 1980 . 3 Page 4 5
| Attitudes and beliefs about diarrhoea: the mother's role |
To drink or not to drink
Jon Rohde discusses the importance of mothers' attitudes
towards drinking in the setting up of an effective oral rehydration programme. While the scientific community continues its debate on the ideal composition, packaging
and delivery of oral rehydration solution, many mothers continue to withhold fluid from
children with diarrhoea. And why not? They know that when a child with diarrhoea is given
extra fluid to drink he passes yet more liquid messy stools. This is true even with the
most modem rehydration mixtures. Although oral rehydration does save lives, its widespread
use will be determined by complex cultural and social factors which are little influenced
by scientific advances. We must understand the beliefs conditioning response to diarrhoea
before an effective strategy can be developed to promote oral rehydration. Local beliefs
Until now, a scientific approach has been used to market ORT, based on three main
points:
- diarrhoea is an illness
- it may be dangerous or even fatal
- one effective modem remedy exists that can be drunk to overcome this danger.
Social marketing, however, has to start with the consumer. In marketing oral
rehydration we must first understand the attitudes of the mother and design our product
accordingly. Interviews with 254 mothers in a rural Javanese community revealed that:
- diarrhoea is not considered an illness but a normal occurrence in the young child's
life.
- it is surely not dangerous, for all young children suffer multiple episodes of diarrhoea
and most of them continue to live in reasonably good health.
- appropriate medicine and visits to a health centre are not considered necessary for a
condition which is not accepted as one of ill health.
Seen in this light, it is hardly suprising that our scientific arguments for OR have
little relevance in rural Java. Marketing a message The usual health education approach is to change the knowledge and attitudes of target
groups, whereas effective marketing strategy is based on the present values and practices
of the consumer. Such a strategy should avoid challenging traditional beliefs as far as
possible - only questioning them where they are definitely incompatible with the marketing
objectives.
|
It is drinking in response to
diarrhoea that is the key element of oral rehydration.
WHO photo by P. A. Pittet We must be absolutely clear about the product we are marketing; precisely what do we
want the consumer to do? It is drinking in response to diarrhoea that is the key element
of oral rehydration. We do not necessarily need to change the concept of what diarrhoea is
or even the fact that it is potentially dangerous. Once the concept of drinking is
accepted in the society then it is relatively easy to discuss what is the best drink in
the circumstances.
|
 |
Strategy
Different concepts of diarrhoea drawn from several cultures suggest a variety of
marketing possibilities. The health profession has tied its marketing strategy for ORT
exclusively to the last example on the chart. However. a majority of health workers
interviewed in Indonesia subscribed to views one, two or three in preference to seven,
despite an extensive re-education campaign by the Ministry of Health over the past five
years. It is obvious therefore - that we must follow the example of the extensive
'jamu'
(Javanese traditional herbal medicines) industry more closely if we are to develop a
successful strategy.
| Local Belief |
Possible Marketing Message |
| 1 Diarrhoea is a cleansing of the body. |
Drink to replenish water, the cleansing element of the body. |
| 2 The body dehydrates and loses strength during diarrhoea. |
Let the body drink to give strength. |
| 3 Diarrhoea is a normal part of growing up. |
It is time to provide a tonic - extra fluid - to strengthen
the child's developing body. |
| 4 Diarrhoea is a hot illness. |
Respond with a cold drink. |
| 5 Athletes drink extra fluid to replace salt and water lost
in sweat. |
Diarrhoea also causes loss of body salts and fluid. Let your
child regain strength through drinking. |
| 6 Diarrhoea is an old and traditionally known condition of
imbalance in life forces. |
There are many useful traditional remedies for diarrhoea. |
| 7 Diarrhoea is a disease. It kills by dehydration. |
Lives can be saved with the newest remedy - oral
rehydration. |
|
|
DDOnline
Diarrhoea Dialogue Online Issue 2 August 1980 . 4 Page 5 6
| Attitudes and beliefs about diarrhoea: the mother's role |
Communication
|
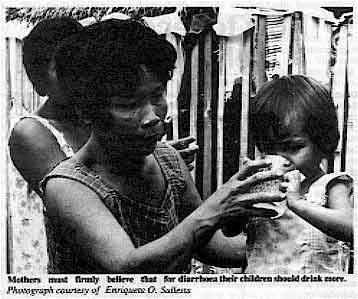
Mothers must firmly believe that
for diarrhoea their children should drink more.
Photograph courtesy of Enriqueta O. Sullesta The message should be communicated to mothers by as many means as possible. Using the
mass media is one obvious way to achieve this, but health planners have rarely maximised
the potential. The " . . . that refreshes" means Coca-Cola all over the world -
has any health message ever been as widely popularized? Successful communication implies reaching decision makers at all levels; this can
sometimes be best achieved through young people.
|
 |
In 1978, a village household survey in central Java revealed a universal withholding of
fluid from children with diarrhoea. Six months later, after primary school teachers had
given simple lessons on preparing and giving home-made sugar-salt solution, 80 per cent of
the heads of these same households advised drinking extra fluid for diarrhoea. (1) Availability and impact It is vital that ORS is widely available before we attempt to market it and that the
campaign reaches as many people as possible. While the effectiveness of oral rehydration
in treating diarrhoea cannot be questioned, its promotion through the formal health system
is likely to reach only a small number of people. But a broad campaign accepted by mothers
at all levels of society to give extra drinking water to children with diarrhoea could in
itself lead to a reduction in dehydration and deaths from diarrhoea. Measuring
Once the idea of drinking more becomes acceptable, the most appropriate fluid must be
chosen depending on cost, availability and the physical state of the child. The next step
may be to provide home-made sugar-salt solution as a technical improvement on plain water.
Finger pinches of salt, various hand or finger measures of sugar and a variety of local
containers such as gourds, coconut shells and tin cans have been tried for standard water
volume. Teaspoons, bottle caps, match boxes and drink bottles, even polythene bags have
all undergone field trials for accuracy and acceptability in measuring the necessary
quantities of sugar, salt and water. Success depends not only on the measuring technique
used, but also on training and the existing socio-cultural conditions. Given even the most
successful strategy for home made solutions there is legitimate concern that mistakes in
preparing such a solution may offset some of the beneficial effects of the improved
rehydration mixtures. Plastic spoon
A further refinement is to provide a more reliable way to make rehydration solution,
such as the two-ended spoon. This was pioneered in Indonesia and shown to be used properly
by the vast majority of mothers there.(2) The cheap plastic spoon may perhaps serve as a
reminder and a stimulus to the mother to provide fluid in both the right composition and
quantity to her child, starting with the earliest sign of diarrhoea. The spoon can carry
the important message not only of how to make the fluid, how much to give, but the
importance of referral to the formal health system if diarrhoea continues for more than 24
hours. Wholesale distribution of such spoons must obviously be accompanied by clear
instructions as to their use. Packets
Village health posts can supply packaged ORS. Mothers initiate rehydration at home
knowing that ORS is available nearby if diarrhoea continues. As demand increases it may
become feasible to expect each household to have its own supply of ORS - although this
would be determined by finance, logistic support and shelf life of the packets. Health
workers are taught to recognize simple signs of dehydration or failure of ORT, assuring
rapid referral to the health centre or district hospital for serious cases. All children
however would receive fluid to drink from the first sign of diarrhoea. Conclusion The attitudes and beliefs of the mother are crucial to the successful use of ORT. Only
through sympathetic understanding of her attitude towards diarrhoea can we develop an
appropriate, acceptable and effective strategy that can rely on her active support. What
to drink and how to make it are of minor importance until mothers firmly believe that for
diarrhoea their children should drink more. (1) Rohde J E, Sadjimin T 1980 Elementary school pupils as health educators: role
of school health programme in primary health care. The Lancet vol 1: 91-92 (2) Hendrata L et al 1980. Pediatrica indonesiana vol 20: 91-92 Jon E. Rohde, formerly at the Rockefeller Foundation, Yogyakarta, Indonesia and now
c/o USAID, Port-au-Prince, Department of State, Washington DC 20521, USA.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 2 August 1980 . 5 Page 6 7
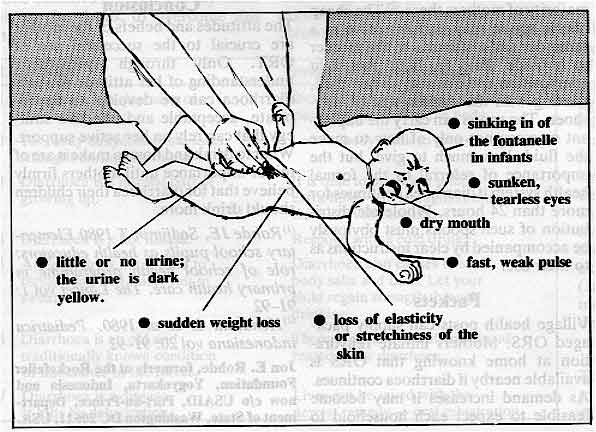
How to recognize dehydration
Diarrhoea kills because it causes dehydration. The stools of a healthy child contain
relatively little water but a child with diarrhoea passes very watery stools which also
contain vital salts (sodium, sodium chloride, potassium and bicarbonate). If the losses
are great, both the water and the salts must be replaced or the child will die. To
recognize the signs of dehydration it is necessary to ask, look, feel and, if possible,
weigh the child. Important signs and symptoms
- Stools Ask about the number and size of the diarrhoea stools. Has there also been
vomiting? These answers may also give clues to the severity of dehydration.
- Thirst This may be the earliest sign of dehydration. Until a child has lost more
than five per cent of his body weight, dehydration causes few signs. When severely
dehydrated, a child may not be fully conscious and may be unable to drink.
- Urine A healthy child usually passes urine about every three hours. The body of a
dehydrated child tries to save water and only produces a small amount of dark coloured
urine. Mothers usually know how much urine their children have passed, so ask them if
there has been less that usual.
- Condition If there is no dehydration, a child will appear alert and well. At a
later stage, he will be weak, irritable and may look unwell or sleepy. A severely
dehydrated child may appear very sleepy or be unconscious. He may also have fits or
convulsions.
- Sunken eyes A child's eyes lie in soft, wet, fatty tissue. If he becomes
dehydrated, this tissue shrinks and becomes drier and his eyes sink back into his skull.
His eyes also lose their shining appearance and stay half open when he is asleep.
- Dry mouth A dehydrated child cannot make enough saliva and so his mouth and
tongue become dry. This is an important sign.
- Breathing Sometimes, a severely dehydrated child breathes fast and deeply. This
kind of breathing occurs when a child has been dehydrated for some days or has been
rehydrated with the wrong fluids. Do not mistake this deep, fast breathing for the
shallow, rapid breathing of pneumonia.
- Loss of skin elasticity The skin of a healthy child is elastic. If you
pinch the skin of the abdomen and then let go, the skin quickly flattens again.
Dehydration makes a child's skin dry and less elastic so when pinched it sticks up for
some seconds before going flat again. If a child is very thin or very fat, loss of skin
elasticity is not easy to detect and therefore not a helpful sign in diagnosing
dehydration.
- Pulse Dehydration makes a child's pulse faster and weaker. When he becomes
severely dehydrated, it may not be possible to feel the pulse at the wrist, you may have
to feel at the groin or listen to the heart. (With very severe dehydration, the pulse is
sometimes slow).
- Sunken fontanelle The fontanelle is the soft place between the bones at the top
of a baby's skull. It is large when he is born but closes over by the time he is about 18
months old. When a baby becomes dehydrated, his brain and tissues in the skull lose water
and shrink. The fontanelle sinks down between the bones of the skull.
- Loss of weight This may occur quickly during a few hours or over several days. A
severely dehydrated child may have lost a tenth or more of his normal body weight. If he
weighed ten kilograms before the onset of diarrhoea, he may have lost at least a kilo of
water and may now weigh only nine kilograms. Loss of weight due to malnutrition occurs
more slowly over several weeks or months.
Conclusion
|
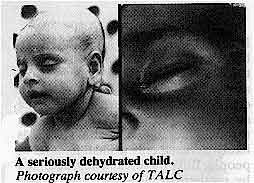
A seriously dehydrated child.
Photograph courtesy of TALC Dehydrated children need urgent rehydration and should be encouraged to drink even if
vomiting occurs. Those with severe dehydration and complications such as convulsions
should be given oral rehydration fluid and taken to a centre where they can receive
special care.
|
 |
|
|
DDOnline
Diarrhoea Dialogue Online Issue 2 August 1980 . 6 Page 7 8
From: Bertrand R. Saubolle, Kathmandu, Nepal.
Thank you for a copy of the first issue of Diarrhoea Dialogue. I am a primary
school teacher in Kathmandu Valley with no medical training. I often walk through a
neighbouring village where I have been struck by the number of people suffering from
intestinal disorders, the commonest being worms, diarrhoea and dysentery. For several
years I have supplied them with Santonine for worms and sulphaguanadine for diarrhoea. As
these poor villagers are not accustomed to medicines, I administer very small doses and
obtain remarkable results. People are cured of diarrhoea in three days, but after a
fortnight they come back for more pills. I have come to the conclusion that it is not the
pills that are required but the absolutely necessary measures of elementary sanitation -
pure drinking water and the use of toilets. Cured people promptly re-infect themselves by
drinking contaminated water. You say on="dd01.htm#page5">page five of the first issue that 'there is
no excuse to stop breastfeeding', With many mothers here, it is not a question of stopping
but beginning breastfeeding. They are so under-nourished that they simply cannot produce
milk. I have seen very young babies being fed on a gruel of rice or wheat, whichever
happens to be in season. The mothers long to breastfeed but they often just cannot. What
is one to do in such cases? I have recommended a varied diet stressing high protein foods
such as eggs, soya beans, lentils and fruit. This is a mockery for the people, however,
who cannot afford a diet like this. They eat a little parched grain and, if they can get
it, rice with boiled nettle or fern tips. Is there any medicine or other means that will
activate the mothers' glands and help them produce milk? For babies with diarrhoea, what
is the use of recommending ORT if the drink is prepared with contaminated water? Mothers
cannot see why they should waste firewood boiling water only to let it cool so that the
baby can drink it cold. What is one to do? I feel frustrated and at the end of my ability.
When one works among the poorest of the poor, what can one do to help without having to do
everything? You raise two important points. How can undernourished mothers produce milk? There is
no magic medicine. Breast milk depends upon the mother's food intake and her body reserves
and it is the baby's sucking which makes the milk flow. The baby should be put to the
breast as soon as possible after birth and encouraged to suck very often even when there
seems to be very little milk. The baby should suck at both breasts every time, starting on
alternate sides, so that both breasts are stimulated as frequently as possible. The
colostrum (the yellowish fluid which is in the breast at birth and during the first day or
two afterwards) is valuable to the baby both as food intake and because it contains
protective substances. It is virtually impossible for a mother not to be able to produce milk for her baby if
the baby sucks frequently enough and if she eats and drinks as much as she can. The family
needs to understand that the mother must eat at least her fair share of the food that is
available because she is feeding both the baby and herself. It is the quantity of food the
mother gets, that is more important than the quality, but adding dark green leaves, some
kind of pulses (peas, beans, lentils etc) and perhaps a little fat such as oil or butter
to the cereal will help. She also needs some extra rest and a great deal of reassurance
and support from all around her - family, friends and health workers. It is of course the mother who should be eating the rice gruel rather than giving it to
the baby. She is much less likely than the baby to develop diarrhoea from contaminated
water or food because she has had time to build up her own natural immunity. If she can
breastfeed even for a few months, she will pass some of her protection on to the baby. Ideally, breastfeeding should continue, with additional foods being gradually given to
the baby after the first few months, for at least two years in the kind of situation you
describe. Family spacing helps too. A birth interval of at least three years gives babies
a better chance of survival in poor circumstances. The mothers can recover more of their
own reserves between pregnancies and breastfeeding. The longer interval also means that
mothers can give the youngest child more care and attention, especially through the
weaning period when other foods are gradually being added to supplement and eventually to
replace the breast milk. About rehydrating with contaminated water - we shall be discussing this in detail in
future issues. The current belief is that bad water is better than no water in diarrhoea.
In your situation do try to keep breastfeeding going, however severe the diarrhoea,
because the milk will provide some protection as well as additional fluid. From: Maurice Bauhahn, Saginaw, U.S.A. Can we have more discussion of the diagnosis of diarrhoea please? A briefly
annotated bibliography on oral rehydration therapy would also be useful. I would also like
to see more emphasis on the villager's problem of wanting and procuring clean water. New knowledge about the pathological agents of diarrhoea will be presented in later
issues of Diarrhoea Dialogue. Detecting these infecting agents is often technically
difficult and expensive. The situation is complicated by the fact that a number of the
organisms associated with diarrhoea may sometimes exist in the bowel without causing loose
stools or disease. Whatever the origin of diarrhoea, the end result is similar; a loss of
water from the body with various amounts of other components and salts. The danger of
diarrhoea is due to this dehydration and the imbalance of electrolytes and body
constituents. Because of this, no matter what the cause, the first action should be to
replace the water lost. The more severe the losses, the more precise should be the
replacement of fluids. There are relatively few cases of diarrhoea in which you need to
know the precise diagnosis in order to give specific medicine or treatment; rehydration is
always the first essential step to be taken. A useful annotated bibliography has now been published by PAHO (see review on="#page2">page 2). Finally, issues four and five of Diarrhoea Dialogue will
concentrate on the relationship between diarrhoea, water and sanitation. The questions on this page have been answered by the editors. In future, we
plan to enlist the help of our panel of editorial advisers and other experts to provide as
extensive an answering service as possible for readers.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 2 August 1980 . 7 Page 8
Oral rehydration I read with interest the="dd01.htm">first issue of Diarrhoea Dialogue discussing
the use of specially prepared oral rehydration packages. However, it seems to me that in
the short term such packages will be too expensive and not readily available for extensive
use in developing countries. I work with a project for strengthening health delivery systems in Central and West
Africa which is based at Boston University. As part of the project, we recently developed
training materials for trainers of village health workers. The materials are currently
being field tested and a final version will be ready sometime in 1981.
|
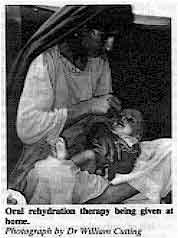
Oral rehydration therapy being given at home.
Photograph by Dr William Cutting One of the main tasks envisaged for the village health worker in these materials is the
education of mothers in the use of oral rehydration. The training materials have been
reviewed by health personnel with wide experience in working in rural areas. They stressed
the need for health education and the use of alternative methods of oral rehydration. The
general need for nutrition education is relation to the treatment of diarrhoea was also
stressed.
|
 |
Sif Ericsson, Health Policy Institute, Boston University, Boston,
Massachusetts, USA. Appropriate and practical
Thank you for sending me a copy of Diarrhoea Dialogue for inspection. I was well
impressed with it. It seems to me that this is the appropriate literature for many people
to have whose concerns are with the many real and practical difficulties of applying not
only oral rehydration but also public health preventive medicines. It seems to me clearly
written and generally sound in content and I wish it great success. D. A. J. Tyrrell, Clinical Research Centre, Division of Communicable Diseases,
Watford Road, Harrow, Middlesex.
Easy reading We have just received the first issue of Diarrhoea Dialogue and I would like to
congratulate you upon it. We are strongly of the opinion that an eight page publication
such as this is likely to be read and the mixture which you have of illustration and news
seems excellent. I think too that your type is easily read which is very important. We
much look forward to receiving future issues. P. J. S. Hamilton, Caribbean Epidemiology Centre, PO Box 164, Port-of-Spain,
Trinidad, West Indies.
Teaching material Thank you very much for sending me the first issue of Diarrhoea Dialogue. I am
writing in response to your question regarding teaching material available in local
languages. I currently have a pilot project area in primary health care involving the use
of young people as well as traditional medicine men as village based primary health care
workers. As one aspect of the project we have introduced the use of special spoons
purchased from Professor David Morley of the Institute of Child Health in London. We have
modified the spoons so that instructions are printed on them in the Iban language. We have
also translated the instruction sheet into Iban, with some additional instructions to
grind rock salt into a fine powder before use and to top up the glass before tasting the
mixture. We have also adapted Jon E. Rohde's story of Abdul and Seri into a local cartoon book
for distribution to the people as well as converting this into an audio visual set for use
in the area. We will be evaluating the use of the spoons and expect to collect samples of the
reconstituted oral rehydration fluid for laboratory analysis. Paul C. Y. Chen, Faculty of Medicine, University of Malaya, Kuala Lumpur 22-11, West
Malaysia.
Successful use of ORT
We are very interested in Diarrhoea Dialogue and would like to continue
receiving it. We have recently visited several countries in the Caribbean to promote oral
rehydration therapy, notably - Belize, Guyana, Antigua, St. Vincent and St. Lucia. An
explosive outbreak of diarrhoea in Antigua was successfully controlled with only four
deaths out of 400 cases using oral rehydration fluid made up in the hospital. Even the
records clerks were rehydrating children. At Bustamante Hospital for Children, the method is now routine and the infectious ward
has been shut, drips have been almost discontinued and mortality is down. With early
re-feeding, hospital stay has been decreased and nutrition improved. Getting it out into
the other areas is a problem because of supplies and training, but we have assisted in one
regional and other national seminars for the Caribbean. The critical factor seems to be
whether or not the area has an interested pediatrician. P. S. E. G. Harland, Department of Child Health, University of the West
Indies, Mona, Kingston 7, Jamaica.
|

Scientific editors Dr Katherine Elliott and Dr William Cutting
Executive editor Denise Ayres
Designer Dick Inglis
Editorial advisory group
Dr I Dogramaci (Turkey)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhorn (USA)
Dr D Mahalanabis (India)
Professor Leonardo Mata (Costa Rica)
Dr Mujibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Dr Paul Vesin (France)
Dr M K Were (Kenya)
With support from WHO and UNDP
|
Issue no. 2
August 1980
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 April, 2014
|






