|
| |
Issue no. 59 - December 1994-February 1995
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-8 Dialogue on Diarrhoea Online Issue 59 - December
1994-February 1995
|
DDOnline Dialogue
on Diarrhoea Online Issue no. 59 December
1994-February 1995  Page 1 2
Page 1 2
Breastfeeding is best feeding
 |
Nutritious and natural: exclusive breastfeeding provides the
best start in life. It is tempting to look to new scientific
discoveries such as the latest vaccines and medicines to reduce child deaths. However. the
very best way to ensure babies grow up healthy is a traditional practice and costs nothing
- breastfeeding.
|
Breastmilk is nutritious and contains antibodies and other substances which protect
against disease. Breastfeeding also reduces the risk of infection associated with poor
food hygiene and inadequate water and sanitation. In developing countries artificially fed
infants are at least 14 times more likely to die from diarrhoea than infants who are
breastfed. Although breastfeeding is promoted in most traditional cultures, urbanisation and
promotion of infant formula are undermining breastfeeding. Exclusive breastfeeding -
feeding infants breastmilk only, with no other foods or fluids - is recommended until
infants are 4-6 months of age. However, breastmilk is often supplemented with other milks
or gruels before infants are ready to be weaned. Health workers' presence at birth and their contact with mothers and infants afterwards
provides them with ideal opportunities to support mothers to establish and continue
breastfeeding. Research has shown that if health workers give skilled support, mothers are
more likely to breastfeed successfully and for longer. This issue of DD looks at the skills health workers need to counsel mothers on
breastfeeding. As well as understanding the techniques of breastfeeding and how to
overcome common difficulties, communication skills such as listening and confidence
building are important. Many women who are in paid employment outside the home think that they will have to
stop breastfeeding once they return to work. However, with good family and workplace
support, this does not need to be the case. Inside, DD suggests several ways
in which women working away from the home can continue to breastfeed. In emergency situations such as refugee camps where access to water, sanitation, food
and health care is very limited, breastfeeding is critical to protecting infant health. In
such settings it is very important to recognise women's ability to breastfeed even in
difficult circumstances and to support mothers to provide the best food for their infants. Finally, this issue looks at what advice to give women in areas where HIV infection is
common. The H1-v virus has been found in the breastmilk of women who are HIV- positive,
and there is a small risk that HIV infection can be passed on to infants through
breastfeeding. However, this risk needs to be balanced against the danger of infants
contracting other serious illnesses such as diarrhoea1 diseases through alternative infant
feeding, especially if families do not have access to clean water and sanitation. William Cutting
|
In this issue:
- Counselling skills Pages 2-3
- Combining paid work and breastfeeding Page 5
- Infant feeding and HIV Page
6
|
|
DDOnline Dialogue
on Diarrhoea Online Issue no. 59 December
1994-February 1995 1 Page 23
Training health care workers to counsel
breastfeeding mothers Felicity Savage and Bernadette Daelmans Daelmans describe a new WHO training course.
Health workers can play a key role in
promoting breastfeeding. Research has shown that if they give appropriate and skilled
support, it is more likely that mothers will breastfeed successfully and for longer.
In the last 20 years knowledge of the scientific basis of lactation and suckling and
about how to prevent and overcome breastfeeding difficulties has increased enormously. But
this new information has not been included in the training of most health workers, leaving
an important gap in their knowledge and skills. To address this. WHO and UNICEF have
developed a 40-hour breastfeeding counselling course designed for health workers who
care for mothers and young children. The course emphasises the development of counselling
and clinical skills to support good breast feeding practices and to help mothers overcome
difficulties according to the new understanding of breastfeeding.
Counselling
For breastfeeding support to be effective, a health worker needs to communicate well with
a mother. Asking too many questions, giving a lot of instructions, or being critical can
make a mother doubt her ability to breastfeed. Instead a health worker needs to listen to
a mother and learn how she feels. Course participants learn the following listening and
learning skills:
- using helpful non-verbal communication (showing your attitude through your posture.
facial expression and gestures)
- asking open questions (questions that require more than just a 'yes' or 'no' answer)
- making responses or gestures that show interest (e. g. nodding or saying 'Aha'
- reflecting back (repeating in different words) what a mother says
- empathising (showing that you understand how she feels)
- avoiding words that sound judging.
Health workers also need to be able to build a mother's confidence and give her
support. Course participants learn six confidence and support skills:
- accepting what a mother thinks and feels
- recognising and praising what a mother and baby are doing right
- giving practical help
- giving a little, relevant information (for example, explaining what has happened or what
to expect)
- using simple language
- making one or two suggestions. not commands.
Clinical skills
Correct attachment of the baby to the breast is important to establish breastfeeding and
to prevent and overcome most common difficulties. Participants learn how, to assess
breastfeeding by looking for the following signs of good attachment:
- the baby' s chin is touching the breast (or is very close to it)
- the mouth is wide open
- the lower lip is turned outwards
- more areola (the circle of dark skin around the nipple) is showing above the baby's
mouth than below it
- the baby takes slow, deep sucks, sometimes pausing.
Next. participants learn how to help a mother to position her baby at her breast so
that the baby attaches well and suckles effectively. There are four key signs of good
positioning:
- the baby's head and body should be in a straight line. not twisted
- the baby should face the breast with his or her nose opposite the nipple
- the mother should hold her baby close to her body
- if the baby is newborn, the mother should support his or her whole body, not just the
head and shoulders.
|
|
Good positioning: the baby takes a mouthful of breast tissue. |
|
|
Poor
positioning: the baby is sucking the nipple only.
|
The same principles apply whether a mother is sitting, standing or lying down to
breastfeed. In the training course. participants help a mother to hold her baby in a good
position and to touch the baby's mouth with her nipple. When the baby opens its mouth
wide. the mother quickly moves the baby onto her breast. aiming the baby's lower lip well
below the nipple. This helps the baby to take a big mouthful of breast tissue including
the milk-collecting ducts under the areola which enables the baby to remove the milk
effectively. Participants also learn how to express milk by hand (see="dd37.htm">DD37) and how to feed a baby by cup (see="dd41.htm">DD41). Participants study and practise the skills in the classroom, then practise applying
them with mothers and babies in maternity wards and outpatients facilities. They learn how
to use these skills to help mothers with common difficulties such as worries that they
cannot produce enough milk, sore nipples, a baby's refusal to breastfeed, engorgement,
breast infections and when a baby is sick or is low birthweight. Dr Felicity Savage, Dr Bernadette Daelmans, CDR, WHO, CH-1211 Geneva 27,
Switzerland. For more information about 'Breastfeeding counselling: A training course' (Ref. WHO/
CDW93.3-6) contact CDR Division. WHO.
|
|
DDOnline Dialogue
on Diarrhoea Online Issue no. 59 December
1994-February 1995 2 Page 34
Counselling in a hospital setting Khwaja Ahmad Abbas reports on a lactation management
clinic in a children's hospital which is helping to increase exclusive breastfeeding. In Pakistan. as in many traditional
cultures, nearly all mothers mish to breastfeed their babies. But exclusive breastfeeding
is not common. Mothers' first milk, colostrum, is usually thrown away, and other liquids
such as water. ghutti (a herbal drink), tea and honey are given to the baby from
birth. Giving other fluids makes a baby suckle less which leads to a decrease in a
mother's milk supply. In order to promote exclusive breastfeeding until 4-6 months of age and to try to solve
mothers' breastfeeding difficulties, a lactation management clinic was started five years
ago at the Children's Hospital in lslamabad. The clinic is run by two specially trained public health nurses who are supervised by a
woman doctor. Infants up to the age of four months and their mothers are referred to the
clinic from other parts of the hospital when they have breastfeeding difficulties.
 |
It is important to ask about the father's and grandmother's
views on breastfeeding, as well as the mother's beliefs, in order to find out the root
cause of a breastfeeding difficulty. |
At the clinic, a nurse asks each mother a standard set of questions to try to find the
cause of the difficulty. As well as a mother's own beliefs, the ideas and the influence of
the child's father and grandmother are taken into account. This is followed by a medical
examination of the mother and baby separately, and observation of the mother and baby
breastfeeding. Close attention is paid to how the baby is positioned and attached, and how
the milk flows. The baby is weighed to check its groivth, mostly to reassure the mother
that her breastfed baby is growing well. As well as giving specific advice (e. g. on solving problems such as sore nipples,
engorgement, mastitis or poor milk production), the nurse encourages mothers to breastfeed
exclusively for 14 months and to continue breastfeeding in addition to giving adequate
complementary foods until two years of age. She explains why bottle feeding and the use of
pacifiers (dummies) are harmful. Each counselling session lasts about 35 minutes. Visual
aids such as flip charts and a life-sized baby doll are used to reinforce the messages.
Mothers are given a pamphlet in the local language to take home. Mothers of young babies who have stopped breastfeeding are assisted with relactation
(see="dd50.htm">DD50 for more explanation). So far, over 4.000 mothers have been counselled at the clinic. More than half of their
breastfeeding difficulties have been caused by poor techniques such as incorrect
positioning. Other important factors have included social attitudes (such as the belief
that if a previous child has died, the mother's milk was to blame). mothers' anxieties or
lack of confidence, incorrect advice from health workers, and low birthweight babies. A sample of 273 mothers are being followed up at home three months after their first
visit to the clinic. Preliminary results show that 67 per cent of mothers had solved their
breastfeeding difficulties. More than 60 per cent were exclusively breastfeeding. while a
further 25 per cent were breastfeeding and still giving other fluids. Only 9 per cent of
those followed up were no longer breastfeeding. These results suggest that lactation management clinics are a useful way of helping
mothers to solve breastfeeding difficulties. Wherever possible similar clinics should be
established in hospitals with maternity and paediatric services. Professor Khwaja Ahmad Abbas, Chief of Paediatrics, Children's Hospital, Pakistan
Institute of Medical Sciences, Islamabad, Pakistan.
|
Steps in lactation counselling
- take the baby's and mother's history, including how the baby is being fed
- examine the baby and mother
- weigh the baby
- observe the mother and baby breastfeeding
- praise the mother for helpful things she is doing
- assess and diagnose the difficulty
- if necessary, help the mother to improve her baby's positioning and attachment at the
breast
- suggest what she can do to overcome her difficulties
- give relevant information, and correct any misinformation
- inform, encourage and motivate the mother and family
- follow up
|
|
DDOnline Dialogue
on Diarrhoea Online Issue no. 59 December
1994-February 1995 3 Page 45
Congratulations to the mothers Mary Fukumoto and Hilary Creed Kanashiro
report on a project where increasing mothers' knowledge about exclusive breastfeeding
was found to be important.
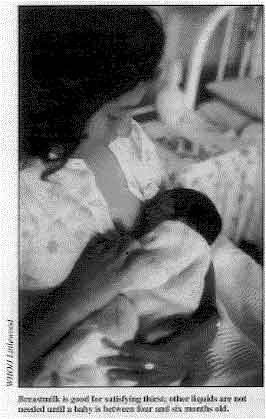 |
Breastmilk is good for satisfying thirst; other liquids are not
needed until a baby is between four and six months old. In the shanty towns of Peru's capital,
Lima, almost all mothers breastfeed their children, but exclusive breastfeeding is rare.
Most mothers supplement breastmilk with herbal teas and many also give other milks. We wanted to know what influences mothers in making decisions about how they feed their
infants. First, we found out local views about early feeding practices and what advice
health workers were giving. We then followed the progress of a group of pregnant women. We
interviewed them in their homes on several occasions: before delivery, as soon as possible
after the birth of their babies, and twice a week until their babies were one month old.
|
We found that decision making about infant feeding is a complex process. A key factor
is mothers' previous experience of feeding infants. Advice from relatives, neighbours and
health personnel is also important. Lack of information about exclusive breastfeeding was common. Nearly all the mothers
believed breastmilk was good for their babies, but they did not know that exclusive
breastfeeding was best. Health workers' understanding was also incomplete. They advised
mothers not to give other milks, but they did not always advise against giving other
fluids such as sweetened water and herbal teas. Mothers commonly believed that they could not produce enough milk for their babies
because they felt they themselves were undernourished. Some believed that although
breastfeeding was good for babies, it could make their own health worse. Other mothers
experienced difficulties with sore nipples when starting breastfeeding. These beliefs led many mothers to introduce other milks to supplement breastfeeding.
Herbal teas were also given because they were thought to prevent and cure colic and
flatulence, and to quench infants' thirst. Based on these findings, the project decided to focus on providing better information
in order to help mothers to produce enough milk, overcome breastfeeding difficulties. and
build their confidence that giving other milks was not necessary. In addition, the project also stressed that breastmilk is good for satisfying thirst
and has benefits similar to herbal teas. Since mothers commonly believe that everything
they eat or drink is transmitted to their babies through breastmilk, they were advised to
drink herbal teas themselves, instead of giving them to their infants. Because breastfeeding practices were so closely linked to mothers' beliefs about their
own needs, the project paid particular attention to mothers, recognising them as valued
people who deserve care and promoting the benefits of breastfeeding for mothers as well as
infants. The slogan for the education -'Congratulations to the mothers, and happy
breastfeeding ' - reflected this. Education was done mainly through showing locally produced videos to small groups of
mothers. Other channels for information included posters, loud-speaker broadcasts from a
mobile van, and the distribution of booklets describing breastfeeding techniques. The educational activities continued for 12 months, so that some women were involved
from when they were first pregnant until the first few months of breastfeeding. The evaluation showed that there was a significant increase in the number of children
aged 0-4 months being exclusively breastfed. However, the improvement had occurred in the
second, third and fourth months. The number of children being exclusively breastfed in the
first month of life had not increased. The increase in exclusive breastfeeding seemed to be a direct result of a decrease in
the use of sweetened herbal teas and waters. The number of women supplementing breastmilk
with other milks did not decrease significantly. This indicates that the intervention was successful in persuading mothers that herbal
teas and waters were not necessary. However, it was more difficult to convince mothers
that they could produce enough breastmilk without needing to supplement it. It suggests
that we need to explore other ways of increasing mothers' confidence.
Dr Marv Fukumoto and Hilary Creed Kanashiro, Instituto de Investigacion Nutritional,
Apartado 18-0191, Lima 18, Peru. The project was supported by WHO's CDD programme.
|
|
DDOnline Dialogue
on Diarrhoea Online Issue no. 59 December
1994-February 1995 4 Page 56
Women, work and breastfeeding Women who work outside the home often assume that they have to stop breastfeeding
when they return to work. Nomajoni Ntombela discusses ways in
which working mothers can continue breastfeeding. Every mother is a working mother, whether
in formal or informal employment, self-employed or working in the home. The UN
Economic Commission for Africa calculates that women carry out up to 75 per cent of all
agricultural work in addition to doing 95 per cent of domestic work. As a result of increasing industrialisation more women are working away from home in
large workplaces such as offices, factories, shops and hospitals. while continuing to take
the main responsibility for child care. Often women working away from home believe that
they cannot continue breastfeeding, although this does not have to be the case. The following are some suggestions about how women can combine paid employment with
breastfeeding.
- Plan your pregnancy so that you can combine maternity
leave with annual leave and spend more time at home with your baby.
- Prepare yourself during pregnancy by learning
about breastfeeding and how to continue breastfeeding when you return to work.
- Ask advice from a friend or relative who has
breastfed; join a breastfeeding support group; talk with a health worker; or read about
breastfeeding.
- Exclusively breastfeed your baby during
your maternity leave.
- When you return to work, continue to
breastfeed your baby whenever you are at home, at night and on days off. If the baby
sleeps in your bed, you can breastfeed more than usual during the night with less
disturbance. Many babies need less milk during the day if they are fed well during the
night.
- If possible take your baby to your
workplace so that you can breastfeed when he or she is hungry.
- Alternatively, ask a helper to bring the baby
to you at work to be breastfed. Or, if your home is not far away, you may be able to go
home during breaks to breastfeed.
- If the suggestions in 6 and 7 are not
possible, it is best to leave expressed breastmilk for a helper to feed your baby while
you are away.
Expressing milk Learn to express your breastmilk soon after the baby is born (see="dd37.htm">DD37).
In the week before you return to work, start feeding your baby expressed breastmilk by cup
during the day. Express your breastmilk early in the morning, so that you are relaxed and not rushed. Most babies need to be fed about every three hours. If possible. express 1/2 cup of
breastmilk for each feed. Many mothers find they can express a total of 2 cups or more.
However, do not worry if this is not possible. If you can only express enough milk for one
feed, then that is still helpful. If necessary, give the baby other milk later in the day. After you have expressed your milk into a clean container, breastfeed your baby. Even
though you have expressed as much milk as you can. your baby will still be able to get
milk from your breast because suckling is more effective than expressing. Cover the container with a cloth and store it in a cool place. Even at room
temperature, expressed breastmilk can be kept for at least eight hours. Teach your helper
how to feed the expressed breastmilk to your baby using a cup. While you are at work, express your breastmilk two or three times during the day. This
will help ensure that your milk production is maintained. If you have access to a
refrigerator at work, the expressed breastmilk can be stored and taken home to feed to the
baby the next day. Household and workplace support Make sure other household members share the workload so that you have more time with
your baby in the morning and when you return from work. Employers have an important role to play in promoting breastfeeding. Supportive
policies should include:
- adequate maternity leave (women should not have to return to work until the baby is at
least four months old and can be given complementary foods in addition to
breastmilk)
- providing a room at the workplace for child care and breastfeeding
- allowing women to have two half-hour breastfeeding breaks
- arranging working hours which enable breastfeeding.
Workers need to negotiate with employers for these conditions. Women should seek
support from their colleagues and workplace organisations such as trade unions to improve
conditions at their workplaces. Nomajoni Ntombela, IBFAN Africa Co-ordinator, PO Box 781, Mbabane, Swaziland.
|
Neli's success story Neli,
a secretary in Swaziland's capital Mbabane, is the mother of three children: aged 10
years, 3 years and 5 months. The youngest, Muziwandile, was born prematurely and weighed
2kg. Neli received counselling on breastfeeding Wing pregnancy and after delivery, and
breastfed exclusively for four months. She negotiated two months paid maternity leave with
her employer and continued to exclusively breastfeed for two months after she returned to
work. Her employer allowed her breaks to express milk at work which a relative collected
and took home to feed to Muziwandile. At four months old Muziwandile weighed 5.5kg. Neli
has since received promotion at work.
|
|
|
DDOnline Dialogue
on Diarrhoea Online Issue no. 59 December
1994-February 1995 5 Page 67
HIV and infant feeding In countries where HIV infection is widespread, some health workers are concerned
about the risks of HIV transmission through breastfeeding. DD discusses the
issues. The HIV virus can be passed from a mother
to an infant. This can happen at three stages: during pregnancy, childbirth or
breastfeeding. However, most infants born to mothers who are HIV-positive do not become
infected with HIV. The HIV virus is found in breastmilk, and some infants are known to have been infected
through breastfeeding. However. it is difficult to assess exactly how much of a risk
breastfeeding is. Few studies have been done, and testing a baby's HIV status is
complicated. Available research suggests that about one in every seven breastfed infants
whose mothers are HIV-positive may become infected by HIV from their mother's
breastmilk. Recent HIV infection or advanced HIV infection mean that a woman has more of the HIV
virus in her body fluids, including breastmilk. Therefore a baby is more likely to
be infected if his or her mother was infected with HIV during pregnancy, childbirth or
breastfeeding, or if she is ill with AIDS related illnesses. Despite this risk, it is important to remember that most women are not infected with
HIV. and that most babies breastfed by HIV-positive mothers do not become infected through
breastmilk. Also, if the baby is already HIV-positive (having been infected in the womb or
during childbirth), breastfeeding will help him or her to stay healthier longer. If a woman knows she is HIV-positive, it is important to help her decide whether the
chance of passing HIV to her baby via breastfeeding is greater than the risks associated
with artificial feeding. For many HIV-positive women, the risk of their babies dying if
not breastfed will be much greater than the risk of passing on HIV.
|
What is HIV? The human immunodeficiency virus (HIV) attacks the body's immune (defence) system,
weakening the body's ability to fight off illness. Many people with HIV stay well for some
time, but eventually their bodies become unable to fight off illness. In the later stages
of HIV infection, people usually develop a group of infections called acquired immune
deficiency syndrome (AIDS).
|
Advice to all women (whether or not they know their HIV status)
- Health workers should discuss the benefits of breastfeeding with all pregnant women.
It is also important to give information about how HIV and other sexually transmitted
diseases (STDs) are spread. The best way to prevent transmission of HIV and other STDs is
by supporting women to protect themselves from unsafe sex, and by encouraging men to take
more sexual responsibility. Women need to know that having safer sex (using condoms or abstaining from intercourse)
is especially important during pregnancy and breastfeeding. If a woman's HIV status is not known
- The vast majority of women do not know their HIV status, and are probably not infected
with HIV. They should be encouraged to breastfeed.
In most communities HIV counselling and testing services are not available, so many
women do not have the choice of finding out their HIV status. However, if a reliable
testing and counselling service is available. a woman may want to discuss whether to have
an HIV test. Counselling helps a woman to prepare for the possibility of knowing that she is
HIV-positive, and means that she can agree freely to a test. The risk of infection through
breastfeeding should never be used as a reason to put pressure on a woman to take
an HIV test. Knowing her HIV status may help her make the decision about whether or not to
breastfeed, and will, of course, affect other choices about her life. If a woman knows she is HIV-positive
- If a woman is HIV-positive, in some situations (especially is she
herself is ill) it may be better for her not to breastfeed, but to find alternatives.
However, alternatives may not be easily available or a woman may decide that the benefits
of breastfeeding outweigh the possible risk of transmission of HIV.
Health workers should help a woman to discuss the implications of being HIV- positive,
and to make an informed choice. Find out what the woman already knows about HIV infection
and breastfeeding, clarify any misunderstandings, and explain the possible risks and
benefits. Reassure her that. whatever choice she makes, she is not to blame if her baby
becomes ill. Issues to consider include:
- Does she have access to clean water? Can she afford fuel or electricity for sterilising
feeding utensils?
- Does she have support from family or friends to help her prepare and give alternative
feeds?
- Does she have access to animal milk? Is there a nearby shop which regularly stocks
formula milk?
- Can she afford to feed her infant with animal or formula milk? In many situations it
will be safer and more feasible to breastfeed.
Alternatives to breastfeeding Infant formula is the most common alternative.
However it is expensive, and hygienic preparation and feeding can be difficult in many
households. To feed an infant for six months. at least 44 tins of 500g are needed. Animal milk, such as cow or buffalo milk, can also be given. Animal milk should be
diluted and sweetened (one cup of water, three cups of milk, four teaspoonfuls of sugar).
It also needs to be brought to the boil to reduce the amount of curd and kill potentially
harmful germs. Giving expressed sterilised breastmilk is another option. Bringing breastmilk to the
boil or pasteurising it (heating to 62.5 degrees centigrade for 30 minutes) kills HIV as
well as other organisms. In some places, it is usual for another woman, often a relative, to breastfeed a baby
if the mother is unable to do so. This option can be considered. but is not advised in
areas where HIV is common since there is a possibility that this other woman may be
HIV-positive. This article is a shorter version of one in AIDS Action 27. For readers who want
more information write to AHRTAG for a copy of the AA article.
|
|
DDOnline Dialogue
on Diarrhoea Online Issue no. 59 December
1994-February 1995 6 Page 78
Breastfeeding in emergencies Marion Kelly proposes a strategy to support
breastfeeding in emergency situations where good infant feeding is crucial to survival.
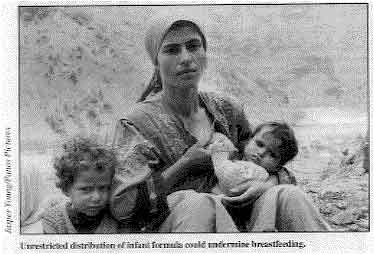 |
Unrestricted distribution of infant formula could undermine
breastfeeding.
People affected by wars or natural
disasters often have to live in crowded and insanitary conditions. Their access to food
and health care services may also be restricted. In these settings. the danger of
diarrhoea and other infections is great. This means that during emergencies breastfeeding
becomes even more important in protecting infant health.
|
Experience of relief operations in a range of countries has shown that anxieties about
breastieeding were most common in countries where artificial feeding was widespread before
the emergency began. Even during war and famine in Ethiopia and Sudan, inability to
breastfeed was much less commonly reported than in recent emergencies in Iraq, Eastern
Europe and the former Soviet Union. This difference suggests that cultural factors are more important in influencing
breastfeeding than the emergency itself. As countries become more
industrialised,
artificial infant feeding is often introduced and breastfeeding skills tend to be lost. In
many cases, inaccurate and out-of-date information about breastfeeding replaces
traditional knowledge. For example. it is often said that poor diet or psychological stress can make a
mother's milk 'dry up'. However, this is not supported by evidence. Although a good diet
is important for the health of mothers themselves, even women who are quite undernourished
are capable of producing enough milk to breastfeed their babies. Psychological stress can
temporarily prevent the release of milk from the breast, but it does not affect milk
production. If suckling continues and a mother's confidence in her ability to breastfeed
is not undermined, then breastmilk will soon flow normally again. Failure to understand this has led to a mistaken belief that during emergencies large
supplies of infant formula are needed to save lives. However, unrestricted distribution of
breastmilk substitutes can undermine breastfeeding and increase the risk of disease and
death. Although almost all mothers are physically capable of breastfeeding, some mothers may
give up or never start breastfeeding if they do not receive encouragement, support and
appropriate advice. Also, all pregnant and breastfeeding women need extra food in order to
protect their own health. Those who provide health care and relief assistance during emergencies should take the
following measures to support breastfeeding and protect the health of mothers.
- Work to get agreement between outside agencies and local health workers on breastfeeding
policy and practice. Share up-to-date information on breastfeeding with those who do not
have all the facts. Establish mechanisms to ensure that all of the following actions are
implemented in a co-ordinated way.
- Make sure that maternity care practices follow the WHO/ UNICEF guidelines. 1
- Do not condemn or criticise women who are not breastfeeding. Instead, take a positive
approach by encouraging mothers to choose breastfeeding and reassuring them of their
ability to do so.
- Educate the whole community about the benefits of breastfeeding. Highlight the
importance of family and social support for breastfeeding.
- Offer one-to-one assistance for mothers who experience difficulties with breastfeeding.
This can be done by helping local women to set up a network through which new mothers can
pet practical advice and moral support from other mothers who have successfully breastfed.
Another option is to train women to work as breastfeeding counsellors. In either case.
those who provide support must be sensitive to the culture, health beliefs and
circumstances of the mothers they assist.
- Provide assistance with relactation to mothers of infants who have stopped breastfeeding
early (see="dd50.htm">DD50).
- Supply adequate basic food rations to every family. Target supplementary food to
pregnant and breastfeeding women and to children of weaning age, not to young infants.
- Only provide infant formula to infants who do not have access to
breastmilk. Remember
that such infants are usually few in number, and take care to identify them correctly.
Make sure that their care givers have the knowledge, skills and resources to prepare and
give feeds hygienically, using cups rather than bottles.
Marion Kelly, Lecturer in Public Health, Centre for International Health, University
of Wales College of Medicine, Heath Park, Cardiff CF4 4XN, UK. 1 'Protecting, promoting and supporting breastfeeding: the special role of
maternity services' is available free from local offices of WHO and UNICEF or by writing
to WHO publications, CH-1211 Geneva 27, Switzerland. Further reading: Write to AHRTAG for a copy of Kelly, M, 1993. Infant feeding in
emergencies, Disasters 17 (2): 110-121.
|
|
DDOnline Dialogue
on Diarrhoea Online Issue no. 59 December
1994-February 1995 7 Page 8
Misleading promotion of breastmilk substitutes For many years health organisations have been campaigning to stop the baby food
industry undermining breastfeeding. In 198I the World Health Assembly adopted the
International Code of Marketing of Breastmilk Substitutes, which aims to regulate
marketing practices for artificial infant foods. It covers artificial milks for babies,
other artificial infant food. and feeding bottles and teats. The code specifies:
- no advertising of these products to the public
- no free samples to mothers
- no promotion of products in health care facilities. including no distribution of
free or low-cost supplies
- no company sales representatives to advise mothers
- no gifts or samples to health workers
- no words or pictures promoting artificial feeding
- all information on artificial infant feeding, including on labels, should
explain the benefits of breastfeeding and the dangers of artificial feeding
- unsuitable products such as sweetened condensed milk should not be promoted
for babies.
So far 11 countries have passed national laws to enforce the code and many more are in
the process of drafting legislation. However despite this, free or low-cost
supplies continue to be provided to hospitals, clinics and individual doctors in many
countries. It is crucial that health workers actively promote breastfeeding and do not allow the
distribution of free or low.-cost formula, other substitutes or bottles and teats in their
workplaces. When breastmilk substitutes are distributed in health facilities, many mothers
believe that health workers recommend these products and that they must be good for their
infants. For more information about the International Code of Marketing of Breastmilk
Substitutes, please contact the World Alliance for Breastfeeding Action (WABA), Code
Compliance Task Force, PO Box 1200, 10850, Penang, Malaysia. Breastfeeding resource list For information about publications and health education materials on breastfeeding and
details of organisations in over 50 countries supporting breastfeeding, write to AHRTAG
for a copy of Breastfeeding Information Resources. The resource list is free to
people in developing countries; for readers elsewhere it costs £5.
|
Obituary - Dr Katherine Elliott DD and AHRTAG regret to announce the death from cancer on 11 November 1994 of Dr
Katherine Elliott. DD's Scientific Editor and AHRTAG's founder. In 1979 Dr Elliott had been approached by Dr Halfdan Mahler, the then Director- General
of WHO. to publish an international newsletter to spread the news about the effectiveness
of ORT. Dialogue on Diarrhoea was born in 1980 and in the 14 years
since has been widely acclaimed internationally, growing to a circulation of over a
quarter of a million readers in nine languages. Dr Elliott set high standards for DD and
made sure that the newsletter recognised the important role of the mother and the family
in promoting child health. DD's success in reaching health workers at district
level with practical advice expressed in plain language was the spur to the publication of
AHRTAG's other newsletters, ARINews, AIDSAction, CBRNews and Health Action. Twelve years ago, WHO estimated that 5 million children died every year as a result of
diarrhoeal diseases. Recent studies suggest that deaths have decreased to 3.2 million a
year. The information and enthusiasm of DD have played an important role, and this
is an appropriate memorial to Katherine Elliott. But she would be reminding us about the
remaining millions, and urging us to play our part! Dr William Cutting, Co-founding Scientific Editor
|
New child health newsletter As a result of feedback from readers about the need for information on a range of child
health issues, AHRTAG is combining its two newsletters Dialogue on Diarrhoea and ARI
News in mid 1995. The new child health publication will continue to provide up-to-date information about
diarrhoeal diseases and acute respiratory infections, and will broaden its focus to
include other key child health topics such as malaria and measles. The last issue of Dialogue on Diarrhoea will be in March 1995. Readers of DD will
automatically be put on the mailing list to receive the new child health newsletter.
|
Readers competition: Help AHRTAG to find a name for its new child health newsletter. Send suggestions for
new names to AHRTAG by 1 March 1995. Prizes for the best entries!
|

Scientific editor Dr William Cutting
Executive editor Kate O'Malley
Design & production Ingrid Emsden
Information support Coral Jepson Editorial advisory group
Kathy Attawell (AHRTAG sabbatical)
Professor A G Billoo (Pakistan)
Professor David Candy (UK)
Dr Shanti Ghosh (India)
Dr Michael Gracey (Australia)
Dr Adenike Grange (Nigeria)
Dr Nicole Guérin (France)
Dr Norbert Hirschhorn (USA)
Dr Sharon Huttly (UK)
Dr Claudio Lanata (Peru)
Dr Jon Rohde (USA)
Professor Dang Duc Trach (Vietnam)
Professor Andrew Tomkins (UK) With support from AID (USA), Charity Projects (UK),
Ministry of
Development Cooperation (Netherlands), ODA (UK), UNICEF, WHO Publishing partners
BRAC (Bangladesh)
CMAI (India)
CMU (China)
Grupo CID (USA)
lmajics (Pakistan)
National Institute of Hygiene and Epidemiology (Vietnam)
ORANA (Senegal)
RUHSA (India)
Turkish Medical Association (Turkey)
Consultants at University Eduardo Mondlane (Mozambique)
|
Issue no. 59 December 1994 - February 1995
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 August, 2019
|






