|
| |
Persistent Diarrhoea
Clinical Update: A supplement to Issue no. 48 - March 1992
pdf  version
of this Issue version
of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-4 Persistent Diarrhoea
A supplement to Dialogue on Diarrhoea Online
Issue 48 - March 1992
|
DDOnline Persistent
Diarrhoea supplement to DD48  Page 1 2
Page 1 2
Clinical Update PERSISTENT DIARRHOEA
Persistent diarrhoea is becoming recognised as an important child health problem
in developing countries, although its control and prevention have received less attention
than acute diarrhoea. This special DD insert reports on the main conclusions of a
meeting held in Mombasa, Kenya in 1991, which presented an overview of the problem and an
update on research about appropriate treatment.
Persistent diarrhoea is an important cause of illness and death in children in
developing countries. Moreover, as acute diarrhoea is more widely and successfully treated
with oral rehydration therapy (ORT), the proportion of diarrhoea deaths associated with
persistent diarrhoea will probably increase. In the mid-1980s the World Health
Organization recognised that efforts to control persistent diarrhoea were inadequate.
Several studies have since been carried out, aimed at formulating strategies for its
management and control. What is persistent diarrhoea? Acute and persistent diarrhoea are not two separate diseases but form a continuum. Most
episodes of diarrhoea last less than one week, but a small proportion of episodes last for
two or more weeks. The definition of persistent diarrhoea has varied, but it is helpful to
have a standard one so that different studies can be compared, and recommendations made
for treatment. In 1987, a meeting sponsored by WHO defined persistent diarrhoea as an
episode which starts acutely but which lasts at least 14 days. This definition has been
adopted by most investigators and programmes. Is it a serious problem? In 8 community based studies in Asia and Latin America (see="#Table 1">table 1),
persistent diarrhoea accounted for between 3 per cent and 23 per cent of all cases of
diarrhoea. In 7 studies (see="#Table 2">table 2) the incidence of persistent
diarrhoea varied greatly. For every 100 children aged 4 years or less, 7 cases of
persistent diarrhoea were seen per year in India, and 150 cases in northeastern
Brazil. In all studies the incidence was much higher in children under 2 years than in
older children. Persistent diarrhoea may account for a large proportion of all deaths due to diarrhoea.
WHO and UNICEF estimated that in 1991 persistent diarrhoea accounted for only 10 per cent
of diarrhoeal episodes, but as many as 35 per cent of diarrhoeal deaths in children under
5 years of age. Evidence from studies in Bangladesh, India, Peru and Brazil indicated that
approximately 45 per cent (range 23 per cent to 62 per cent) of diarrhoea associated
deaths were due to persistent diarrhoea. Although findings from some studies indicate that persistent diarrhoea most often
occurs in children below 2 years of age, most persistent diarrhoeal deaths occur in
children aged 1 to 4 years old when malnutrition is most common, because deaths from
persistent diarrhoea are frequently associated with malnutrition.
|
Table 1: Duration of diarrhoeal episodes
|
|
| Country |
Age (years |
Total Episodes |
Percentage of episodes by duration |
| 1-7 days |
8-14 days |
15+ days |
| Indonesia |
0-1 |
618 |
83% |
14% |
4% |
| Guatemala |
0-1 |
262 |
53% |
27% |
19% |
| Peru |
0-1 |
1,299 |
79% |
14% |
7% |
| Peru |
0-2 |
5,302 |
88% |
9% |
3% |
| Bangladesh |
0-4 |
941 |
66% |
21% |
14% |
| Bangladesh |
0-4 |
2,609 |
71% |
22% |
7% |
| Bangladesh |
0-5 |
1,074 |
50% |
27% |
23% |
| India |
0-5 |
471 |
35% |
55% |
10% |
|
Table 2: Incidence (per 100 child-years)
of persistent diarrhoea by age group
| Country |
Age group |
| <1 year |
1 year |
2 years |
3 years |
4 years |
Overall(0-4) years |
| India |
31 |
9 |
6 |
2 |
0 |
7 |
| Nepal |
15 |
17 |
12 |
10 |
14 |
| Peru |
31 |
22 |
16 |
- |
- |
26 |
| Bangladesh |
72 |
25 |
29 |
28 |
6 |
34 |
| Bangladesh |
58 |
57 |
55 |
39 |
33 |
48 |
| Bangladesh |
64 |
74 |
67 |
43 |
59 |
| Brazil |
171 |
216 |
160 |
90 |
60 |
150 |
|
References: Table 1: Indonesia (1), Guatemala (2), Peru (3), (4), Peru (5), Bangladesh (6), (7), Bangladesh (8) , Bangladesh (9), India (10). Table 2: India (10), Nepal (11), Peru (5), Bangladesh (8), Bangladesh (9),
Bangladesh (12), Brazil (13). Produced by Dialogue on Diarrhoea and the Applied Diarrhoeal Disease Research Project
(ADDR), Harvard institute for International Development, Cambridge, MA 02138, USA
|
|
DDOnline Persistent
Diarrhoea supplement to DD48 1 Page 2 3
What causes persistent diarrhoea? A number of studies have tried to find out if particular pathogens are associated with
persistent diarrhoea. This information could help to predict the course of the disease and
help decide whether to use an antibiotic. However, most cases of persistent diarrhoea seem
to be associated with the same pathogens that cause acute diarrhoea. Four studies in India, Bangladesh and Peru found that rotavirus.
Aeromonas, Campylobacter, Shigella and Giardia lamblia were equally common in acute and
persistent diarrhoea. Cryptosporidium was more common in persistent than acute
diarrhoea in Bangladesh, but the reverse was true in Peru. Evidence from several studies
suggests that the entero-adherent Escherichia coli (so called because of their
ability to adhere to intestinal cells in tissue culture) may be particularly associated
with persistent diarrhoea. However. these organisms may be responsible for only a small
proportion of all episodes. Even though most pathogens seem to be equally common at the onset of acute episodes
that do or do not become persistent, different pathogens are found if cultures are taken
from the same individual during the course of persistent diarrhoea. Studies in Bangladesh
and Peru showed that it was not common to find the same pathogen in samples taken at
different times during a persistent episode. The current evidence therefore suggests that
no single pathogen is responsible for the persistence of episodes. Moreover, successive
infections with different pathogens often occur in children with persistent diarrhoea. What increases the risk of persistent diarrhoea? Several factors have been identified as possibly increasing the risk of persistent
diarrhoea.
- Previous diarrhoea infection
A relatively small proportion of children have many episodes of diarrhoea, and it is
predominantly these children who develop persistent diarrhoea. This observation is
supported by studies which show that a recent diarrhoeal illness is often associated with
the occurrence of persistent diarrhoea. More studies are required to find out whether
these, high-risk children are in an environment where there is greater transmission of
enteric pathogens, or if they have greater susceptibility to illness. Studies are also
needed to find out if the frequency of diarrhoea infections affects the child's immune
status and ability to resist subsequent infection.
- Nutritional status
Evidence from Bangladesh, India and Brazil shows that malnutrition is strongly associated
with persistent diarrhoea. Researchers have found a small increased risk of diarrhoea
incidence in malnourished children, but a large increased risk of prolongation of the
episode. In Bangladesh, for example. among persistent diarrhoea deaths, 81 per cent were
associated with malnutrition. These findings suggest that malnutrition significantly
increases the risk of dying in children suffering from persistent diarrhoea.
- Feeding practice
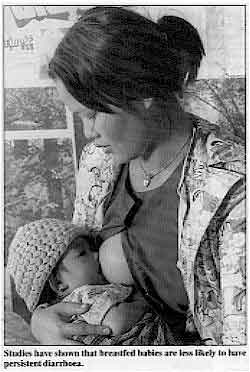 |
Studies have shown that breastfed babies are less likely to
have persistent diarrhoea.
- Studies have shown that breastfeeding shortens the duration of diarrhoeal episodes, and
that lack of breastfeeding is associated with persistent diarrhoea. In Peru, for example,
infants aged from 9 months to 11 months who were not breastfed had average diarrhoeal
durations that were 49 per cent longer than those of infants who continued to receive some
breast milk. One reason for this is that diarrhoea infections can reduce a child's
capability to digest lactose, a sugar found in milk. When this happens, drinking animal
milk can cause diarrhoea to worsen or be prolonged.
|
-
Other factors
Research is continuing on the relation of several other factors to persistent diarrhoea.
These include deficiency of vitamin A, zinc, iron and other micronutrients; behaviours
related to water source and use, food preparation and consumption and hygiene; presence of
other diseases such as measles; suppression of immunity; and the interaction of these
factors.
Other studies have attempted to find out whether clinical characteristics during the
initial days of diarrhoeal illness can predict which episodes are likely to persist.
Results from Peru and Bangladesh show that the initial phases of what became persistent
episodes were more likely to be accompanied by fever, vomiting, high stool frequency,
dehydration and reduced activity in children. However, these associations were not
sufficiently strong to be able to precisely predict which episodes would persist.
|
|
DDOnline Persistent
Diarrhoea supplement to DD48
2 Page 3 4
Treatment
The same general principles apply for treating acute diarrhoea and persistent
diarrhoea. Stool losses should be replaced with appropriate fluids, feeding should
be.continued and unnecessary medicines avoided.
Dietary management is especially important in persistent diarrhoea because of the
association of persistent diarrhoea with malnutrition, lactose intolerance and (probably)
micronutrient deficiency, and because the diet of children with persistent diarrhoea
should be modified so that the intake of animal milk is reduced.
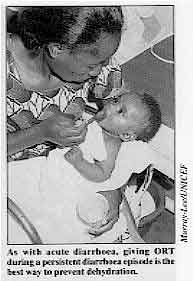
| As with acute diarrhoea, giving ORT during a persistent
diarrhoea episode is the best way to prevent dehydration. The principle of replacing water and electrolyte losses is well established for
acute diarrhoea and is no different for persistent diarrhoea. The aim of treatment is to
replace initial and ongoing fluid losses until the diarrhoea stops. In nearly all cases of
persistent diarrhoea ORT is all that is required for fluid replacement. |
 |
- Dietary management
The association between persistent diarrhoea and malnutrition means that appropriate
feeding is very important during and after the diarrhoea episode. There are two key
principles of dietary management of persistent diarrhoea:
(a) Reduce lactose by decreasing the amount of non-human milk in the diet
Persistent diarrhoea is less common in children who are breastfed than in those who
are given cow's milk or other non-human milks.
Lactose intolerance occurs especially in children who are severely malnourished or who
have severe diarrhoea. Lactose is a sugar providing about 35 to 45 per cent of the
calories in non-human milks used for feeding children. Once in the gut, it must first be
broken down by an intestinal enzyme called lactase, before it can be absorbed by the gut
wall cells. During the early phase of a diarrhoeal episode lactase production may decline,
slowing down digestion of lactose.
If the sick child continues to ingest milks containing lactose, any undigested lactose
passes into the lower intestine, where it can draw fluid from the gut wall cells into the
intestinal lumen, thereby increasing the severity of diarrhoea. Fortunately, clinically
significant lactose intolerance occurs in only a very small proportion of children with acute
diarrhoea.
In a child with persistent diarrhoea, adverse effects can usually be avoided by reducing
lactose intake to about 2 to 3g/kg/day (about 30 to 50ml/kg/day of whole cow's milk) and
mixing the milk with cereal. Replacement of cow's milk by fermented milk products. such as
yoghurt, which contains less lactose, is another way to reduce the intake of lactose.
|
Evaluating the benefits of giving
nutritious food
with a low lactose content
Two studies in Pakistan evaluated the use of:
- (a) a traditional diet - khitchri (rice and lentils cooked with oil) - for
treating children with acute diarrhoea, and
- (b) khitchri and yoghurt for children with persistent diarrhoea.
Khitchri is commonly given to sick children in Pakistan. The first study was carried out to assess the efficacy of khitchri along with
half-strength cow's milk in the treatment of severe acute diarrhoea (1).
This study involved boys aged between 9 months and 4 years old who had had acute diarrhoea
for 72 hours or less, moderate or severe dehydration and no previous antibiotic treatment.
After initial rehydration the children were randomly assigned to two groups. One group received only glucose ORS for 24 hours. The other was
given khitchri as well as glucose ORS. The intake of food, fluid and glucose ORS
and the output of stool and urine were measured and recorded: 44 children were
successfully treated, 21 with ORT and 23 with khitchri.
 |
Children in Pakistan with persistent diarrhoea showed a significant improvement when
fed on a traditional diet of khitchri. After 24 hours there were no significant differences between the two groups in mean
stool output, frequency of stools or weight gain. These data indicate that the khitchri
diet was well tolerated and did not cause increased stool output in young children
with acute diarrhoea.
|
Successful local diet The second study evaluated khitchri combined with yoghurt in the management of
persistent diarrhoea (2). The study compared soy formula milk (which has
no lactose) with a khitchri-yoghurt mixture in boys aged between 6 months
and 3 years old. Yoghurt is widely used as a dietary supplement in Pakistan and is well
absorbed, mainly because the lactose content of milk is reduced by half by fermentation.
Soy milk was used in the control group because a diet low in lactose is often advised
during persistent diarrhoea. Children with persistent diarrhoea were randomly allocated to the two treatment groups:
khitchri with yoghurt, or soy formula. During the first week of the study, despite
a comparable intake of calories, children fed the khitchri-yoghurt diet had lower
stool volume, lower stool frequency and greater weight gain than children on soy formula. Children on soy formula were switched to khitchri-yoghurt during the
second week. Their weight gain during this week was significantly greater than during the
first week. In addition to the advantages of clinical efficacy and convenience, the potential
financial benefits of a diet based on local foods are also great. The weekly cost of the
soy formula (which is mostly imported) is about $14.00 for a 5kg child compared with only
$2.00 for khitchri- yoghurt. The difference, when multiplied by the many episodes
of persistent diarrhoea treated each year, could result in large financial .savings for
the whole country. These studies provide one example of a local diet using rice, lentils
and yoghurt which can be successfully used for the dietary management of both acute and
persistent diarrhoea.
|
|
DDOnline Persistent
Diarrhoea supplement to DD48 3 Page 4
(b) Ensure that the child receives enough nutritious food
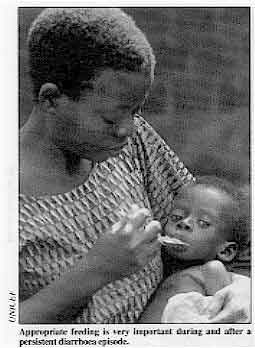 |
Appropriate feeding is very important during and after a
persistent diarrhoea episode. A second essential aspect of the dietary management of persistent diarrhoea is to make
sure that adequate food intake is maintained. As most children with persistent diarrhoea are cared for in the community by the
family. recommendations for dietary management should be based on foods that are
inexpensive, readily available, culturally acceptable, and easy to prepare in the home.
Special diets, such as formula milks that are free of cow's milk or lactose, are too
expensive for most families in developing countries, and are rarely needed.
|
Recent studies have shown that both acute and persistent diarrhoea can be successfully
managed with diets based on local staple foods. But the diet for those with persistent
diarrhoea should have the animal milk content reduced or mixed with other foods. Studies in several countries are evaluating the efficacy of their local diets in
managing persistent diarrhoea. A multi-centre study to evaluate a treatment scheme for
persistent diarrhoea using local foods is now underway in six countries with the support
of the Applied Diarrhoeal Disease Research Project and the World Health Organization
Programme for Control of Diarrhoeal Diseases. These studies are based on the principle of
reducing the proportion of lactose in diets to treat persistent diarrhoea. Children in
Pakistan are given a diet of khitchri (rice and lentils cooked with oil) with
yoghurt: children in Peru, India, Vietnam and Bangladesh are given a rice-milk diet; and
children in Mexico are given a maize-milk diet. Children who do not recover on the initial
diet are switched to a second diet, which contains no milk, such as one diet based on rice
mixed with a protein source, for example chicken or egg white.
- Drugs
Antibiotics should not be used in persistent diarrhoea except for certain specific
pathogens. Shigella is known to cause persistent diarrhoea and can be treated with
antibiotics: antibiotics should be used when Shigella is isolated by stool culture or when
the stool is bloody. Non-specific antibiotic therapy, given without knowing what is
causing the diarrhoea episode, has not proved to be effective against persistent
diarrhoea and should not be used.
Besides antibiotics, a number of other drugs have been tried in the management of
persistent diarrhoea. Cholestyramine and bismuth subsalicylate have shown benefit in some
studies, but are not recommended for routine use. Antimotility drugs (codeine. paregoric,
tincture of opium, diphenoxylate and loperamide) have serious side effects and should not
be used. Adsorbants such as kaolin, smectite and charcoal are also unlikely to be
effective.
Why treatment sometimes fails Although 80 per cent of children with persistent diarrhoea may be managed with proper
feeding and ORT, it is important to be able to identify children for whom such treatment
is likely to fail or recovery may be delayed. In Pakistan treatment failure was more
likely in younger children and those who were vomiting; delayed recovery was associated
with younger age, malnutrition and severe watery diarrhoea. In Bangladesh children with
more severe diarrhoea were also more likely to have delayed recovery. Key issues for future research Although many aspects of the development of persistent diarrhoea are unclear. its
strong association with malnutrition and high incidence and fatality rates in developing
countries, suggest that it deserves much more attention. Information is needed on:
- Locally available diets that can be used for initial treatment and for treatment
failures, so that practical treatment schemes can be developed in different settings.
- The role of immune factors in the persistence of some episodes and the recovery from
diarrhoea.
- The role of micronutrients in treating persistent diarrhoea and improving growth.
- Care-seeking behaviour during acute and persistent phases of diarrhoea, and the
relationship of care-seeking and treatments used to the outcome of the episode.
1. Shaikh S, et al.. 1991. A traditional diet as part of oral
rehydration therapy in severe acute diarrhoea in young children. J. Diar,: Dis. Res. 9:
258-263.
2. Bhutta Z A, et al., 1991. Dietary management of persistent
diarrhoea: comparison of a traditional rice-lentil based diet with soy formula. J.
Ped.
88: 1010-1018.
These studies were carried out at the Aga Khan University and the National Institute
of Child Health in Pakistan, arid supported by the Applied Diarrhoeal Disease Research
Project (ADDR) of Harvard University. Acknowledgements This supplement is based on material prepared by Drs Fitzroy Henry, Jonathan
Harrington and Robert Black of the Applied Diarrhoeal Disease Research Project which is
funded by USAID and managed by the Harvard Institute for International Development, in
collaboration with the Johns Hopkins School of Public Health and Tufts New England Medical
Center. The international meeting on persistent diarrhoea held in Mombasa, Kenya in January
1991 was sponsored by the ADDR project and the WHO CDD Programme. The following are references for the studies cited in this insert. 1. Joe L K, et al., 1966. Diarrhoea among infants in a crowded area
of Jakarta, Indonesia. A longitudinal study from birth to two years. Bull WHO 34: 197-210.
2. Mata L J, et al., 1967. Diarrhoeal disease in a cohort of
Guatemalan village children observed from birth to age two years. Trop & Geogr Med 19:
247-257.
3. Lopez de Romana G, et al., 1989. Longitudinal studies of
infectious diseases and physical growth of infants in Huascar, an under-privileged
peri-urban community in Lima, Peru. Am J Epidemiol 129: 769-784.
4. Black R E, et al., 1989. Incidence and aetiology of infantile
diarrhea and major routes of transmission in Huascar, Peru. Am J Epidemiol 129: 785-799.
5. Lanata C F et al., 1991.
Epidemiologic, clinical and laboratory
characteristics of acute vs persistent diarrhoea in peri-urban Lima, Peru. J Ped Gastroent
and Nutr 12: 82-83.
6. Black R E, et al., 1982. Longitudinal studies of infectious
diseases and physical growth of children in rural Bangladesh. I. Patterns of morbidity. Am
J Epidemiol 115: 305-314.
7. Black, R E, et al., 1982. Longitudinal studies of infectious
diseases and physical growth of children in rural Bangladesh. Am J Epidemiol 115: 315-324.
8. Baqui A H, et al., in press. Epidemiological and clinical
characteristics of acute and persistent diarrhoea in rural Bangladeshi children. Acta Paed
Scand.
9. Henry F J, et al., in press. Epidemiology of persistent
diarrhoea and aetiologic agents in Mirzapur; Bangladesh. Acta Paed Scand.
10. Bhan M K, et al., 1989. Descriptive epidemiology of persistent
diarrhoea among young children in rural northern India. Bull WHO 67(3): 281-288.
11. Laston S, 1992. Risk factors for diarrhoeal disease in village
children in Nepal. Doctoral dissertation, Case Western Reserve University
12. Huttly S R A, et al., 1989. Persistent diarrhoea in a rural
area of Bangladesh: a community based longitudinal study. Int J Epidemiol 18:964-969.
13. Schorling J B, et al., 1990. A prospective study of persistent
diarrhoea among children in an urban Brazilian slum: patterns of occurrence and aetiologic
agents. Am J Epidemiol 132: 144-156. Produced by Dialogue on Diarrhoea and the Applied Diarrhoeal Disease Research Project
(ADDR), Harvard Institute for International Development, Cambridge, MA 02138, USA
|
Persistent Diarrhoea
Clinical Update - A supplement to Issue no. 48 March 1992
Page Navigation
This edition of Dialogue on Diarrhoea Online is
produced by Rehydration Project.
Dialogue on Diarrhoea was published four times a year in English,
Chinese, French, Portuguese, Spanish, Tamil, English/Urdu and Vietnamese and
reached more than a quarter of a million readers worldwide.
The
English edition of Dialogue on Diarrhoea was produced and distributed by
Healthlink
Worldwide.
Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any
uses made of the material.
|
updated: 4 March, 2016
|






