|
| |
Issue no. 14 - August 1983
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-8 Diarrhoea Dialogue Online Issue 14 -
August 1983
|
DDOnline
Diarrhoea Dialogue Online Issue 14 August
1983  Page 1 2
Page 1 2
Meeting the demand
The challenge to the world set out at the recent International Conference on Oral
Rehydration Therapy (ICORT) is summarized on="#page2">page two. All at ICORT
agreed that oral rehydration is a simple, cheap, effective and acceptable way to prevent
millions of children dying unnecessarily from dehydration due to diarrhoea. The value of
immunization programmes and improved nutrition was also stressed, but no good reason was
given to delay making ORT available everywhere. All possible resources ought to be
harnessed to reach this target within the next few years. Diarrhoea Dialogue has now entered its fourth year of publication and such a
powerful consensus of opinion from the ICORT meeting provides welcome support for the idea
behind the newsletter. In this issue we look at some of the contributions that the mass
media and the concept of 'social marketing' can make towards getting the oral rehydration
message across at every level. These forces offer much in the way of influence and
outreach but there needs to be caution about when, where and how they are used. If the
demand for ORT is created, then the means for ORT must be to hand. Not readily available
It is a sobering thought that fizzy drinks and cigarettes seem to reach the remotest
places, when letters to Diarrhoea Dialogue (see="#page8">page eight in
this and previous issues for just a few examples) suggest that packets of ORS, or even the
simple ingredients for homemade oral rehydration fluids, are not always readily available. Nevertheless, we cannot postpone meeting this most basic health need. Rapid and
imaginative action is required on the part of some governments to provide at least a
minimum health care infrastructure to cope with the demand. Essential skills required
Skills in logistics, training and management are as essential as the communication side
of the oral rehydration enterprise and it may now be necessary to look beyond the
conventional channels for quick and efficient assistance. There is now a real prospect
that far fewer children need to die of diarrhoea. Planning, policy-making and delivery of
ORT must receive priority, or the hope that has been created may fade in disappointment. K.M.E.
 |
Isolated community in the Sudan. ORT has to be made available in even
the most remote places.
|
|
In this issue...
- Mass media in the promotion of ORT
- Health education for non-literate audiences
- Rotavirus ten years on
|
|
DDOnline
Diarrhoea Dialogue Online Issue 14 August
1983 1 Page 2 3
ICORT The International Conference on Oral Rehydration Therapy (ICORT) was held in Washington
DC in June. The meeting was sponsored by USAID, in cooperation with the International
Centre for Diarrhoeal Disease Research (ICDDR, B), UNICEF and WHO. For four days it
brought together more than 500 people from over 100 countries. The real value of the
conference lay in the interchange of experiences and the almost complete agreement reached
about the efficacy of ORT and the need for immediate action to make it internationally
available. ICORT identified a number of key areas requiring immediate action:
- Educational programmes must be improved and expanded so that those best placed to
prevent dehydration - mothers and families - are well informed on how to do this.
- Serious research must be carried out into the possible nutrient enrichment of oral
rehydration fluid.
- Alternative carbohydrate substrates for the fluid and even traditional fluids such as
carrot soup require proper investigation.
 |
Mothers must understand how to prevent dehydration. Here,
a Honduran mother learns how to mix Litrosol (see article on pages="#page4">4
and 5). The meeting stressed the importance of convincing health professionals of the value of
ORT and the spin-off effect this would have in terms of improved training about ORT for
other health workers and in re-orienting medical and nursing school curricula. Another major recommendation made was the improvement of cooperation with other sectors
outside the health service to provide the necessary infrastructure to promote and provide
ORT. A key part of this process would be the improvement of communication and extensive
use of the mass media within integrated health education programmes.
|
ICORT's sponsors want positive action to double the use of ORT worldwide each year from
now on. The way to make ORT work is through practice not theory. Further delays in
promoting its use are unjustified while so many children are dying for lack of a drink. Facing the problems
Diarrhoea has been identified as a major problem and ORT a vital intervention by both
WHO and UNICEF. The agencies have underlined their concern and continuing commitment to
reducing infant mortality and morbidity due to diarrhoea by issuing an important joint
statement.(1) The document does not go into the. practicalities of preparing and
administering ORT, which have been dealt with in other WHO publications (2 & 3). It
considers ORT in the broader context of national primary health care programmes and
stresses the extent to which a strong infrastructure (health education, supporting
services and supplies) is essential if ORT is to become more widely available. A key
factor in this process is the promotion of ORT in the community using every available
means. The number of sachets of oral rehydration salts (ORS) currently produced around the
world is only sufficient for about two per cent of all episodes of diarrhoea. With this in
mind, the statement stresses the importance of correct and early use of home solutions to
prevent dehydration and when ORS is unavailable. The challenges include identifying
and publicising the most suitable home solution in each area, increasing the production
and availability of ORS and extensive promotion of both options to as wide an audience as
possible. (1) The management of diarrhoea and use of oral rehydration therapy. A joint
WHO/UNICEF statement. 1983.
(2) A manual for the treatment of acute diarrhoea. 1980.
(3) Guidelines for the trainers of community health workers on the treatment and
prevention of acute diarrhoea. 1980.
Available from: Diarrhoeal Disease Control Programme, WHO, 1211 Geneva 27,
Switzerland.
|
In the next issue...
We will review the topic of feeding and
diarrhoea. Which are the best foods to give and why is breastfeeding so important? We will
also consider the possibilities for nutrient enriched ORS. |
|
DDOnline
Diarrhoea Dialogue Online Issue 14 August
1983 2 Page 3 4

|
The success of a
pilot study using ORT for outpatients encouraged the Ministry of Health in Jamaica to set
up a National Diarrhoeal Disease Programme. Results from its Phase I (1980-82) show that
definite strides have been made towards reducing mortality and the need both for admission
to hospital and the use of intravenous fluids.
|
Oral rehydration therapy has been integrated into the primary health care system, using
auxilliary health workers as part of health centre teams which are supervised by a doctor,
nurse/practitioner or nurse. Initially, supervisors and other key personnel are taught how
to train others in the practical skills of ORT, communication and health education. At the
health centre, parents learn how to use ORS and how to recognize the signs of dehydration.
They are given packets for further use at home, together with advice about the
re-introduction of solid food. Pamphlets, posters and radio programmes reinforce the
educational message. To achieve qualitative as well as quantitative success as the programme expands,
Jamaica plans to improve the health information system to obtain more reliable data for
use in evaluation and in policy-making about appropriate home intervention. Supervision
and management are also to be improved. Communication between health workers and parents
at health centres is recognized as being sometimes inadequate. Giving out ORS without
proper instructions is not enough; and good advice about nutrition is also essential.
Community education will soon begin and this should help to strengthen the programme still
further, particularly in relation to the promotion of breastfeeding and other nutritional
improvements. Book reviews Low cost printing for development
by Jonathan Zeitlyn This handbook helps people design materials and do their own printing. It also includes
information on how small-scale publications can be well printed at low cost with locally
available technologies. The book hopes to encourage local production of educational
materials appropriate for the communities where they are to be used. It draws extensively
on the author's work in India but also reflects ideas and experiences from many other
parts of the world. The material is divided into four separate booklets making up a
handbook of 120 pages. There are many drawings, diagrams and examples of printing from
different countries. The handbook costs £4.00 (plus 45p for surface postage). If you
would like a copy write to: Jonathan Zeitlyn, 51 Chetwynd Road, London NW5, United
Kingdom. Oral Rehydration Therapy: An Annotated Bibliography
(Second edition 1983)
Edited by Michael J. McQuestion
Pan American Health Organization The second, updated edition of this valuable bibliography is now available from the Pan
American Health Organization. A large amount of new material has been added to the
bibliography covering a wide range of topics, including clinical trials, composition of
ORS, impact of ORT on morbidity and mortality rates and implementation of ORT programmes. The bibliography costs $6.00 and is available from the Pan American Health
Organization, 525 Twenty Third Street, NW, Washington DC 20037, USA
|
|
DDOnline
Diarrhoea Dialogue Online Issue 14 August
1983 3 Page 4 5
| Promoting ORT: integrating mass media, print and visual aids |
Delivering the goods
Many communities are still unaware of the benefits of ORT. The Ministries of
Health in Honduras and The Gambia have taken up the challenge and are promoting ORT
through an integrated educational campaign. William Smith
reports on this exciting initiative. Since 1981, a widespread educational programme - the Mass Media and Health Practices
Project* - has been underway in Honduras and The Gambia, showing thousands of
villagers how to recognize the signs of dehydration and to prepare and give oral
rehydration therapy (ORT) correctly at home. These two countries were chosen because of
their contrasting cultures and environments, to make it easier for techniques developed to
be used in other countries later on. By combining specially designed radio programmes,
simple graphic materials and targeted advice for health workers, the governments of both
countries are using mass media to improve the delivery of ORT services, showing that
semi-literate communities can be taught to mix and give ORT safely. Unique approach In both Honduras and The Gambia, village attitudes, beliefs and practices guided the
project design. Mixing trials, home observations, focus groups and individual interviewing
helped select the key audiences and define the most effective educational messages. Each
country has developed its own unique approach to ORT delivery and village education. In
Honduras, the government is providing locally produced oral rehydration salts called
Litrosol for both home and clinical use. In The Gambia, packets are available at health centres but a simple sugar and salt
solution is also promoted for home use because it is too costly to make the packets
available in every home. The Gambian medical and health departments developed a standard
formula for this home-administered solution, using a local soft drink (Julpearl) bottle
and cap for measurements. One litre of fluid is made up from three Julpearl bottles
of water, eight caps of sugar and one cap of salt. The correct way of preparing and giving
the solution was broadcast to mothers on Radio Gambia (the national radio station).
Printed material was distributed to reinforce the message and health workers talked with
mothers to make sure they had understood. Radio
Radio is an important aspect of the Mass Media Project in both countries because
it reaches more people, more quickly and more often than any other medium being used. It
has four particular purposes:
- Convincing rural people that diarrhoea is a serious problem.
- Teaching and reminding them how to mix the oral rehydration solution.
- Answering common questions identified during village visits.
- Leading people to sources of additional help.
In both Honduras and The Gambia, many people own radios so these can be used
effectively for public education. The Mass Media Project's radio broadcasts in The
Gambia are chatty and informal conforming with popular programming style there. The
broadcasts answer health questions quickly and accurately and open a dialogue with
mothers. The Gambian government has provided free time for hundreds of diarrhoea-related
messages on Radio Gambia. In Honduras, the project took advantage of a large network of commercial radio
stations. The radio spots were short and catchy and intended to compete with high quality
commercial advertisements. The featured spot, a 60 second song, became a nationally
popular tune. Follow-up announcements emphasized child care during diarrhoea, encouraged
administration of Litrosol and stressed the importance of continuing breastfeeding during
diarrhoea. Graphics
The graphics used by the Mass Media Project to illustrate the health messages
are simple and clear. The main materials interact directly with the radio messages and
health workers to teach the important skills of mixing and giving oral rehydration
solution at village level. This is particularly important in The Gambia because rural
women are unfamiliar with printed material of any kind and need help with interpreting
pictures. It was necessary, for example, to develop an appropriate visual way of showing
the difference between sugar and salt and illustrating the Julpearl bottle and cap
needed for correct measurement. A colourful 8" x 11" poster was developed which
shows the bottle and cap being used to mix the rehydration solution. The "mixing
pictures" of sugar, salt, and water are colour coded and linked to explanations given
over the radio. In Honduras, early field research indicated that mothers associated child care with
loving images. This attitude was shown visually by a large red heart surrounding a picture
of a breastfeeding woman. The heart was also later associated with Litrosol and a young
family added to the picture to reinforce the role of the husband in giving ORT. Integration of communication techniques
The project's radio programmes strengthened the visual symbols in both countries
through special jingles and romantic songs about motherhood, as well as providing basic
information.
|
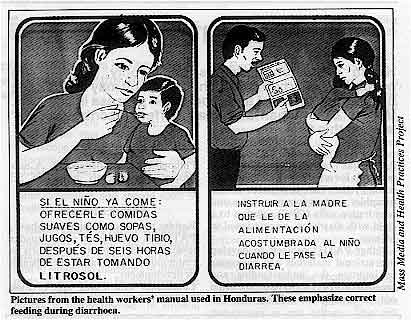
Pictures from the health workers' manual used in Honduras.
These emphasize correct feeding during diarrhoea.
In Honduras, for example, the programme told mothers where to get Litrosol, how to mix
it in the proper volume of water and how to measure it in containers easily found
everywhere. Radio was also used to identify a special network of health workers and
village contacts - red heart ladies - who had been trained to mix
Litrosol. Some
1,200 red heart ladies flew a red heart flag above their homes to attract village
women to this local resource. The integration of the different methods of communication is
a key feature of the Mass Media Project.
|
 |
|
|
DDOnline
Diarrhoea Dialogue Online Issue 14 August
1983 4 Page 5 6
| Promoting ORT: integrating mass media, print and visual aids |
Happy baby lottery
To encourage more Gambian mothers to participate in the project and to maximize the
integration of radio, printed material and input by health workers, a national contest was
launched to popularize the home-administered rehydration solution. Known as the Happy
baby lottery the contest helped to begin the distribution of some 200,000 "mixing
pictures" to mothers throughout the country. Radio Gambia broadcast repeated
programmes to rural mothers on how to use the posters as entry tickets for the contest.
The programmes also taught mothers how to interpret the mixing instruction on the poster.
Health workers were trained to use the posters to teach mothers how to mix the formula as
well as giving UNICEF ORS packets to severely dehydrated children in rural clinics. Village contests
Distribution of the posters was followed by a month of 72 village contests. Every week,
the radio announced the names of 18 villages to be visited by a judge wearing a 'happy
baby' t-shirt. To enter the contest, mothers went to the nearest village displaying a
happy baby flag and, if they mixed the solution correctly, won a prize - either a plastic
litre cup or a bar of locally made soap. These prizes were chosen because they were
appealing, locally available, inexpensive and consistent with project goals. The cup, for
example, is a common container for drinking water and a convenient one litre measure for
the sugar and salt solution. The response to the lottery was enthusiastic. More than 11,000 mothers attended the
village contests. Over 6,500 entered the mixing competition, while hundreds more watched,
listened and learned the new advice on treating diarrhoea. Winning mothers' names were
included in a later draw for 15 radio-cassette players. A single community prize of rice
and sugar was given each week for the village turning out the most mothers for the
contest. Radio was used regularly to publicize the winners and to reinforce the mixing
formula. The lottery ended when the Gambian president's wife drew and announced the names
of the grand prize winners in a special radio broadcast. The lottery is only one part of the Gambian government's use of mass media to fight
infant diarrhoea. Special happy baby flag ladies, like those in Honduras, have been
trained to give mixing advice to village women. Regular radio broadcasts include
traditional songs, drama and popular personalities to explain the dangers of dehydration
and to stress the importance of breastfeeding during diarrhoea. Conclusion
There has been an encouraging acceptance of ORT in both countries. During the first 12
months of the project in Honduras, half of the mothers reached were using
Litrosol. In The
Gambia, after eight months of the campaign, half of the mothers reported using the
recommended sugar and salt solution to treat diarrhoea. An extensive three year evaluation
is continuing in both countries. Three elements have been critical to the success of the project:
- Education and an effective delivery system
An effective delivery system for the UNICEF packets and instructions on the sugar/salt
mixing were combined with practical and widespread education on how to use the new remedy.
- Flexibility
Regular information from the field was used to make changes in methods and materials so
that mothers' questions could be quickly answered.
- Rural beliefs and traditions
formed the basis for the educational campaign.
Resources are available to provide modest assistance to other countries interested in
developing a mass media programme of this sort. Much has yet to be learned, but a
systematic use of mass media integrating radio, print and dialogue between health workers
and mothers can significantly improve the outreach of many health education programmes. Further information on the project is available from Dr William Smith, Vice-
president, Academy for Educational Development, 1414 Twenty-second Street, NW, Washington
DC 20037, USA. * The project is sponsored by the Office of Education and Office of Health, Bureau
for Science and Technology, US Agency for International Development.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 14 August
1983 5 Page 6 7
Simple but not easy
Health education materials using only pictures are needed in many countries. The
end result may look simple but the development and production process is complex. Margot
Zimmerman and Joan Haffey describe
PATH's* work in
this field. PATH has been preparing illustrated materials for non-literate audiences for several
years. Their first health-related pamphlet, on how to mix and give oral rehydration salts
(ORS) solution to a child with diarrhoea, was designed in Mexico. Other PATH* projects to develop instructional materials and packaging to improve the
understanding and acceptability of ORS have been carried out in Bangladesh, Indonesia, the
Philippines, and Thailand (1). A new project was recently begun in Sri Lanka. Broader lessons
Besides the detailed guidelines above, PATH has also learned some broader lessons.
These apply to any efforts to communicate information about health or development. Continuous field-testing and revision
As materials are prepared, continuous field testing and revision with the intended
audience are essential to ensure that the materials are understood and serving their
purpose. Multi-level approach
When introducing a new product or method, a broad approach to providing information to all
those who will come in contact with it is best. Doctors, nurses, fieldworkers etc. all
have different information needs, and materials should be appropriate to the services they
perform and what they need to do their work more effectively. Involving the national programme early
A pilot project that is developing materials intended for use on a wider scale must
involve the final distributor of the materials at a very early stage. PATH has seen from
its own experience that failure to do this can prevent even successful materials from ever
being used throughout a country. Government staff must feel a part of the project. This
also helps to ensure that elements of the message or materials design will be appropriate
to mass distribution. Unexpected findings
Project staff should realize that this work can lead to unexpected findings. While
evaluating the Mexican ORS pamphlet, it was found that, despite the scepticism of both US
and Mexican staff conducting the research, both men and women preferred a version of the
pamphlet showing active involvement of the father in the care of the sick child to one
with only the mother. New projects will teach new lessons to target audiences and staff
alike. National self-sufficiency
Pilot projects that develop information materials by using the methodology described here
also serve a broader purpose: project staff will be learning skills that build a national
expertise in producing other information materials. This can lead to national
self-sufficiency in this type of education and communication.
|
Guidelines for production From its work in this field PATH has developed guidelines for the production of
instructional material for non-literate communities:
- Keep pictures as simple as possible. A crowded scene will divert attention from the
message being conveyed.
- Though excessive detail interferes with understanding of the message, comprehension may
also be reduced by over-simplication.
- Content must be limited to the most important messages. Only 8-12 major points can be
effectively covered in a single pamphlet.
- Each picture and each page should have a single, sharp meaning.
- Visual symbols should be as realistic as possible.
- Pictures are more likely to be successful if faces, clothing and buildings are based on
what is familiar locally.
- Use only familiar objects and symbols to portray a message. For example, many different
kinds of light sources could be used to signify night (a light bulb, a kerosene lamp, a
candle, a metal lamp). The symbol chosen must be tested with people from the intended
audience to ensure it is appropriate.
- Material produced for national distribution may not be equally appropriate for all
regions of the country.
- The ideal length for a pamphlet is usually 16 pages. This often corresponds both to the
space necessary to depict 8-12 major messages and to the attention range of most readers.
It is also usually the most economical format for high-speed printing presses.
- Initial print runs should be small, even if the cost per copy is higher, so that changes
can be made following further evaluation and before mass distribution.
- Understanding of the picture is greater when a person's whole body, rather than just
part of it, is illustrated.
- If the material will be printed in more than one colour or will include simple words,
these choices should be pretested in the same way the illustrations are tested. Remember
that certain colours have different meanings in different societies.
- Using colour at all also adds to the production cost, an important point to remember.
- Non-literate people do not necessarily look at pictures in the order intended. As
messages are being tested, it is useful to ask several groups of people to arrange them
into the sequence that seems most logical to them.
- The design and testing of simple materials are more complicated and require much more
time than the development of written materials. Simple does not mean easy.
- The intended audiences should always have the final say about the content,
illustrations, and sequences used.
- Not all kinds of technical information can be transferred through illustrations.
Pictures can probably be used to teach someone how to change a motorcycle tyre, but it is
doubtful they can be used to teach a person to drive that motorcycle.
|
Margot Zimmerman and Joan Haffey, PATH, Canal Place, 130 Nickerson
Street, Seattle, Washington 98109, USA. *PATH - the Program for Appropriate Technology in Health. (1) Reprints of a paper describing these projects, "ORS: Promotion of
Acceptability and of Safe and Effective Use," are available from PATH.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 14 August
1983 6 Page 7 8
| Acute childhood diarrhoea |
Searching for viruses
Ten years after her first description of rotavirus in The Lancet, Dr
Ruth Bishop reviews current research on the commonest cause of acute
diarrhoea in young children. Viruses are now known to be the most common infectious agents causing acute diarrhoea
in young children. Ten years ago, most diarrhoea in young children had no known cause. No
bacterial or viral pathogens could be isolated from as many as 80 per cent of patients.
Our understanding of enteric infection increased enormously when the electron-microscope
was used to search for viruses that would not grow in cell culture. Electron-microscopy of
diarrhoeal faeces identified at least five new groups of viruses. These are Norwalk
viruses (and other small viruses), rotaviruses, enteric adenoviruses, asroviruses and
coronaviruses.
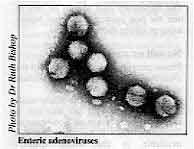 |
Enteric
adenoviruses Although these viruses are very different in appearance, they probably all infect and
partially destroy the outer layer of cells lining the small intestine. The death of. these
cells results in the loss of a large volume of fluid and electrolytes and this causes
acute diarrhoea. Without treatment, children die from dehydration.
|
The ability of the small intestine to digest and absorb food is reduced both during and
for some time after diarrhoea. However, absorption of oral rehydration solution (ORS) is notseriously affected and it is essential that children continue to receive the amounts
of the solution required. Simple new test
These new viruses are all very difficult to grow in cell culture. For this reason, most
of the research done during the past ten years has occurred in laboratories that have an
electron-microscope. Diagnosis of rotavirus infection can now be made by an ELISA test
(see="dd11.htm#page5">Diarrhoea Dialogue 11, page 5).
This is a fairly simple and rapid procedure and should soon be available as a diagnostic
kit. Importance of hand-washing
Rotaviruses are the most important group of viruses, and cause 30 to 80 per cent of
childhood diarrhoea in different parts of the world. In countries with cold winters,
rotavirus infection is mainly a winter disease. In tropical countries with little seasonal
variation in climate, rotavirus infections are common all the year round. Rotaviruses are
very infectious and survive for long periods of time in the environment. They are present
in diarrhoeal faeces in very large numbers and spread from person to person probably by
faecal-oral contamination. They can also contaminate water supplies. Careful attention to
hand-washing by parents, nurses and doctors should help to prevent rotavirus spreading in
families and in hospitals. Value of ORT and breast milk
Rotavirus infections occur at all ages but are most severe in young children 6 to 24
months old. Most babies are protected at birth from severe rotavirus disease by antibodies
received from their mothers, particularly in breast milk. Diarrhoea due to other viruses
is usually less severe. Viral diarrhoea can be treated in the same way as cholera and
early oral rehydration will prevent death due to dehydration. Rotavirus infection occurs
early in life and most children possess rotavirus antibodies by 2-3 years of age. This
does not mean that they are immune to further infection. In fact is seems likely that
everyone is repeatedly reinfected with rotaviruses throughout life. Small groups of
children have been studied carefully from birth to 2-3 years of age and some have had more
than one attack of rotavirus diarrhoea during that time. However, the second attack has
often been milder than the first. Further research necessary
These studies need to be repeated in children in tropical countries. We also need to
find out whether mixed infections (with other enteric pathogens and parasites) increases
the severity of rotavirus diarrhoea. There are many strains of rotaviruses throughout the
world. They change from year to year, and do not seem to last in a community for more than
two years. Fortunately only four serotypes of rotaviruses have so far been identified. It
is not yet known whether infection with one serotype immunizes children against infection
with other serotypes. The most exciting recent development occurred when Japanese research workers succeeded
in growing human rotaviruses in cell culture. This will make it possible to grow and
compare rotavirus strains from many different countries (1). Other enteric viruses
In comparison with rotaviruses, disease caused by other enteric viruses is less severe.
Viruses of the Norwalk group are widely distributed throughout the world and are a common
cause of diarrhoea in young children. But the diarrhoea is milder and may not result in
high mortality, even in developing countries. There is little information about worldwide
distribution of astroviruses and they have not yet been reported in children in developing
countries. Again, they seem to cause comparatively mild diarrhoea in young children.
Enteric adenoviruses can cause severe infection in young children. An ELISA test to
diagnose adenovirus infection has recently been developed in Sweden and this should make
it possible to study how common they are in developing countries.
|
Coronavirus particle
Research into coronaviruses is still at an early stage and proof is still required that
particles seen in diarrhoeal faeces by electron-microscopy are in fact viruses.
Coronavirus-like particles have been reported in many children with acute diarrhoea in
Vellore in India, and in faeces from Aboriginal children in Central Australia. They may
prove to be a very important cause of diarrhoea, particularly diarrhoea associated with
established malnutrition.
|
 |
Conclusion The past ten years have seen exciting and rapid developments in understanding the
causes of acute diarrhoea in young children. If treatment, especially rehydration therapy,
is available rapidly to young children it is possible to reduce the high mortality due to
acute childhood diarrhoea in developing countries. In the long term it is hoped that a
rotavirus vaccine will be produced that will immunize children safely and effectively, and
that this vaccine will also prevent much of the malnutrition that is associated with
diarrhoea. Dr Ruth Bishop, Department of Gastroenterology, Royal Children's Hospital,
Parkville, Melbourne, Victoria 3052, Australia. Editors' note: A future issue of Diarrhoea Dialogue will review progress in developing vaccines
against viruses causing acute diarrhoea. (1) Sato K et al 1981 Isolation of Human Rotavirus in Cell Culture. Archives of
Virology, Vol. 69 155-160. Further reading: Bishop R F 1981 Viral Gastroenteritis in Medical Microbiology and Infectious
Diseases edited by Braude A Z et al. W. B. Saunders, London.
Bishop R F et al 1983 Clinical Immunity after Neonatal Virus Infection. N Eng J Med 309:
72-6.
Estes M K and Graham D Y 1979 Epidemic Viral gastroenteritis. Amer J Med 66: 1001-1007.
Holmes Z H 1979 Viral gastroenteritis. Prog Med Virol25: Z-36.
Steinhoff M C 1980 Rotavirus. The first five years. J Pediat 96: 611-622.
Tyrrell A J and Kapikian A Z 1982 Virus infections of the Gastrointestinal tract. Marcel
Dekker, New York.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 14 August
1983 7 Page 8
We three, i.e. an Ayurvedic doctor, a field botanist and a medical
social worker, work among the tribals of Karjat Taluka, Raigad District in Maharashtra
State of India. Our main aim is to strengthen the traditional health system based on
medical plants existing in the area for primary health care. On the basis of our studies,
we have found many strengths in the local health system and we must promote and increase
the knowledge of the local practitioners. Diarrhoea is rampant in our area. We strongly feel an intensive educational campaign
will help the situation. Where could we get good audio visual aids for this disease in
India? Ours is a Marathi speaking community. Is it advisable to give ready-made packages
or ask the mothers to prepare a solution. The mothers do not have potassium chloride,
baking soda etc. Nancy Gaikwad, Academy of Development Science, Kashele Taluka, Karjat District,
Raigad, Maharashtra 410201, India.
The Voluntary Health Association of India (VHAI) has materials on diarrhoeal
diseases and ORT. You could also contact Dr Vijay Kumar who has produced various
materials on this subject for use in the community. If you can obtain packets of ORS easily - either from local sources or from UNICEF
in New Delhi - you can build your health education programme around them. Otherwise, you
will need to teach mothers how to prepare a simple sugar-salt solution at home, to be
given very early on in diarrhoea to prevent dehydration. A basic recipe uses eight level 5
ml teaspoonfuls of sugar and one level teaspoonful of salt mixed thoroughly in one litre
of clean water. A cupful of this fluid should be given to the child for every loose stool
passed. Do not worry if potassium chloride or baking soda are unavailable. We have sent
you other information about giving oral rehydration therapy. Voluntary Health Association of India
C-14 Community Centre
Safdarjung Development Area
New Delhi 110016,
India Dr Vijay Kumar,
Professor of Community Medicine.
Post Graduate Medical institute,
Chandigarh,
India.
Can liquid ORS be stored safely?
We have stocks of sucrose/glucose, potassium chloride, sodium bicarbonate and sodium
chloride and would like to make our own oral rehydration solution as we find the sachets
quite expensive considering how often they are indicated. Making up a solution suitable for administration involves having large ant-proof
containers; and transporting sufficient stocks to supply an outlying dispensary for a
month or two poses a weight problem. We are at present making up a concentrated solution of which 50 ml is diluted up to a
litre by the dispensary nurse. The concentrated solution is kept in brown two litre
bottles and we are considering weighing out the sodium bicarbonate separately and putting
it in a separate container so that, if the solution has to be stored for more than a
month, it can be added just before sending it out to a dispensary. We use unboiled rain
water for all stages of solution. Bearing in mind the question of bacterial contamination and the reaction of sodium
bicarbonate with glucose can you tell us if the final solution the patient gets is likely
to be an effective rehydration agent. Is such separation of the bicarbonate necessary?
Thank you for your help. David K. Masters, Medical Director, Hospital de la CBPZ, Bolobo, B. P. 397,
Kinshasa, Zaire.
Editors note: We asked appropriate experts to answer the above letter. This is their
reply: We would not recommend storing liquid ORS, whether concentrated or normal strength,
for two reasons. First there is a significant risk of bacterial contamination,
particularly if less than sterile water is used. This is why WHO recommends that ORS
solution, once prepared, should not be kept more than 24 hours. Second, the solution will
become brown because of the interaction of the glucose and the bicarbonate. Keeping the
bicarbonate or sucrose/glucose in a separate container would solve the second problem, but
only until all the ingredients were mixed. If weight is a factor, the concentrated
solution would obviously weigh more than the dry ingredients. We would recommend sending the dry ingredients to the dispensaries rather than a
concentrated solution, with the glucose/sucrose in one packet and the other ingredients in
another, both packets being wrapped together. This double packaging will ensure long shelf
life in areas where usage rates are low. The dispensary staff should be sure to mix the
two packages together before using or giving them to mothers.
No salt or sugar
Please provide us with one copy of the Diarrhoea Dialogue for our MCH clinic and
one for the Hospital itself. Is it possible to get the ready-made diarrhoea sugar and salt mixture in sachets, since
we are so poor here in Tanzania, there is no sugar nor salt available in the whole country
nowadays. Sirkka Kanerva, Assistant Matron, Bulongwa Luteran Hospital, P O Box 42,
Bulongwa,
via Njombe, Tanzania.
We suggest you contact the representatives of UNICEF at P.O.B. 4076 or WHO at
P.O.B. 9292 in Dar-es-Salaam. They will give you information about suppliers of ORS
sachets in Tanzania. If you need further information write to: The Programme Manager,
CDD/WHO, 1211 Geneva 27, Switzerland.
|

Scientific editors Dr Katherine Elliott and Dr William Cutting
Executive editor Denise Ayres Editorial advisory group
Professor David Candy (UK)
Dr I Dogramaci (Turkey)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhorn (USA)
Dr D Mahalanabis (India)
Professor Leonardo Mata (Costa Rica)
Dr Mujibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Professor Andrew Tomkins (UK)
Dr Paul Vesin (France)
Dr M K Were (Kenya) With support from WHO, UNICEF and SIDA
|
Issue no. 14 August 1983
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 August, 2019
updated: 23 August, 2019
|






