|
| |
Issue no. 16 - February 1984
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-8 Diarrhoea Dialogue Online Issue 16 -
February 1984
|
DDOnline
Diarrhoea Dialogue Online Issue 16 February 1984
 Page 1 2
Page 1 2
Diarrhoea and immunization - a valuable ally?
Disentangling the causes of early childhood death in the developing world is
complicated. The="dd15.htm">last issue of Diarrhoea Dialogue discussed
the dangerous partnership between malnutrition and diarrhoeal disease. Improved feeding
and widespread use of oral rehydration will prevent many unnecessary deaths and handicaps
associated with impaired child growth and development. Employing every strategy
The 1984 UNICEF report on The State of the World's Children recommends four techniques
to make a 'revolution for children' a genuine possibility: oral rehydration therapy (ORT);
growth monitoring; expanded immunization; promotion of breastfeeding and better weaning
practices. All these strategies must be brought into play if the revolution is to succeed.
All face similar constraints: cost; lack of local health care infrastructures: the time
and the skills needed to educate families about how they can themselves make best use of
limited resources to improve the quality of life for their children. Shortcuts to bypass obstacles
In any battle, shortcuts to bypass obstacles can hasten overall victory. Measles, like
malnutrition, seems inextricably linked with dangerous episodes of acute diarrhoea in
young children. Two types of measles-associated diarrhoea are recognized. These are
'with-measles diarrhoea' occurring around the time of the illness, and 'after-measles
diarrhoea', occurring sometimes several months later. The diarrhoea mostly appears as
severe dysentery with blood and mucus, rather than the watery type. Infections like
Salmonella and Shigella play a major role and mortality rates are high. It seems that
measles infection lowers childhood resistance to diarrhoeal infections in the environment
and that this effect may persist for a significant period. Less measles may go
hand-in-hand with less deaths from childhood diarrhoea. Effective and economical
Immunization has greatly decreased the incidence of measles among children in western
or more prosperous societies. Measles immunization is now an integral part of the Expanded
Programme on Immunization (EPI), to which many developing countries are committed with the
support of the World Health Organization and UNICEF. There is no doubt that immunization
against the six major infectious childhood diseases - measles, tetanus, whooping cough,
diphtheria, polio and tuberculosis - must greatly benefit child health throughout the
world. Cost is comparatively small for the long term protection. According to the 1984
UNICEF Report, it is approximately five US dollars per child to cover both delivery
systems and vaccines. A cost-effective intervention?
Should measles immunization be urgently pushed as a cost-effective intervention to
reduce the child death rate from diarrhoea? (1) Malnutrition, diarrhoeal and other
childhood infections interact together to kill. Measles immunization must be explored as a
potential shortcut in diarrhoeal disease control and our main article in this issue sets a
South Indian scene for this. Investment bonus for the future
Investment in immunization technologies, training and delivery systems must, in any
event, be a worthwhile use of resources because more effective vaccines against acute
diarrhoeal infections are gradually being developed and their pathways to the periphery
will already be in place. Progress with some new anti-diarrhoeal vaccines is reviewed on
pages="#page3">3 and 7. Some readers may feel too much
space in this issue is taken up with research matters. It may nevertheless reassure other
readers to know that some effective anti-diarrhoea vaccines may become available before
too long. ORT still the front-line defence
Immunization is a preventive, protective intervention. Measles immunization may well
turn out to be a valuable ally in the struggle to reduce diarrhoea morbidity and mortality
among young children in the developing countries. Oral rehydration still remains the
essential front-line treatment for all acute infectious diarrhoeas which cause
dehydration, whether measles-associated or not. KME and WAMC (1) Feachem R. G. and Koblinsky M. A. Bull. WHO. 1983. 61. 641-652. (Reprints from:
Director, CDD Programme, WHO, 1211 Geneva, 27, Switzerland).
|
In this issue...
- Measles immunization in diarrhoeal disease control
- Expectations for a rotavirus vaccine
- Managing local immunization programmes
|
|
DDOnline
Diarrhoea Dialogue Online Issue 16 February 1984
1 Page 2 3
Swing to ORT in Britain
For the last ten years, most babies admitted with gastroenteritis to East Birmingham
Hospital have been treated with oral rehydration. Over 90 per cent of the infants respond
rapidly to the fluid given and can quickly return to their previous diet, whether breast
milk feeds, cow's milk formula, or weaning foods. Infants who are in shock because of
fluid loss, those in whom the diagnosis is unclear or where generalised sepsis is a
possibility, and those too weak to drink are given intravenous fluids. Since about 1977,
children with hypernatraemic dehydration have been treated on our unit with the same oral
rehydration fluid as those with normonatraemic or hyponatraemic dehydration.
Hypernatraemia has not in itself been considered a reason for intravenous therapy. All babies are given a low sodium formula containing approximately 35 mmols of sodium
per litre along with appropriate potassium and bicarbonate or lactate. This is a lower
concentration than that recommended in the WHO formulation. However, in contrast to the
WHO fluid, the formula is given as the only fluid intake, rather than alternating with
free water. We have had no problems with this regimen. Probably the exact composition of
oral rehydration solutions is of considerably less importance than some academic workers
have suggested, except in cases of severe, watery, cholera-like diarrhoea. What is
important is the use of oral rather than intravenous therapy in the vast
majority of babies with acute gastroenteritis. In Birmingham, as in Bangladesh, the use of
oral fluid has revolutionised the management of acute infant gastroenteritis. M. J. Tarlow, Senior Lecturer in Paediatrics, East Birmingham Hospital, Birmingham
B9 5ST, UK.
Hospital practice foreshadows changes in GP prescribing
Between September 1979 and March 1980 Dr Little and his colleagues at a general
hospital in Chatham, Kent studied the 181 children admitted with acute diarrhoea (1).
Three years later, over the same eight months period, they again reviewed the 186 children
admitted with diarrhoea (2). During the first period, not a single case had been treated
with oral glucose-electrolyte solution by the general practitioner before admission. By
1983, at least 10 per cent had received this specific oral rehydration therapy. It is not
clear whether a greater awareness about the value of promoting drinking in diarrhoea was
also associated with advice about increasing the ordinary fluid intake. Other treatment prescribed by the GPs had changed even more. The number who had been
given antibiotics had fallen from 22 to 7 per cent of cases, and those given
'anti-diarrhoeal drugs' like kaolin, had fallen even more sharply from 30 to 5 per cent. (1) Little T M 1981. British Medical Journal, 4: 1300.
(2) Little T M 1983. Personal communication. King Faisal International Prize
This important Saudi Arabian prize in medicine for 1983 has been awarded for work on
diarrhoeal diseases. The outstanding and complementary research success of various groups
has been recognized by equal division of the prize between: Professor John S. Fordtran,
Department of Internal Medicine, Baylor University, Dallas, Texas; Dr William B. Greenough
III, Director of the International Centre for Diarrhoeal Disease Research, Dhaka,
Bangladesh; Professor Michael Field, Department of Pharmacological and Physiological
Sciences, University of Chicago. The triumph of oral rehydration therapy in reducing
mortality and morbidity due to cholera and other acute infectious diarrhoeal diseases is
based on the discoveries of these three scientists and their colleagues over the last 20
years. ICDDR, B Journal
Diarrhoea Dialogue 12 announced the beginning of the Journal
of Diarrhoeal Diseases Research, to be produced and published by the International
Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR, B). The first two quarterly
issues are now available and will be reviewed in Diarrhoea Dialogue
17. Readers may also like to know that the proceedings of an international conference on
'Shigellosis: a continuing global problem'*, held in Bangladesh in 1981, are now available
from ICDDR, B, GPO Box 128, Dhaka 2, Bangladesh. The book will be reviewed in a later
issue of Diarrhoea Dialogue. *The cost is US$ I5.00 (developed countries) and US$ l0.00 (developing countries)
by surface mail. Air mail costs 10 per cent extra in Asia and 20 per cent extra elsewhere. Early immunization against measles?
Measles immunization of young infants in high risk areas may soon be possible using a
new aerosol (nose spray) vaccine. Babies inherit some protection against measles from
their mothers but, where measles is a particularly common and serious infection, this may
not last until the normal age (9-10 months) for immunization is reached. The new vaccine
could be a valuable step forward and results from its field trials will be reported in a
later issue of DD. Sabin A B et al 1983 Successful immunization of children with and without maternal
antibody by aerosolized measles vaccine. Journal of the American Medical Association
(JAMA) 249, 19.2651- New directions
The January 1983 issue of Directions, a newsletter published by the Program for
Appropriate Technology in Health (PATH), is a practical source of immunization-related
information. For a free copy of Directions write to: PATH, Canal Place, 130
Nickerson Street, Seattle, WA 98109, USA. In the next issue
- Breastfeeding - another worthwhile intervention?
- Country reports.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 16 February 1984
2 Page 3 4
Expectations for a vaccine
Tom Flewett considers the prospects for a rotavirus
vaccine and its role in diarrhoeal disease control. It is generally agreed that most acute infectious diarrhoea in young children is caused
by viruses rather than bacteria and it is among young children that most deaths from acute
diarrhoea occur. In many hospital-based studies, as much as 60 per cent of cases of acute diarrhoea are
due to rotavirus infections, but this varies from year to year and from place to place. In
South Africa, only about 15-17 per cent have been attributable to rotaviruses (1). Two
questions arise:
- Is it possible to develop a vaccine capable of preventing this disease?
- Would this rotavirus vaccine make a significant impression on the number of fatal cases
of acute infectious diarrhoea?
Serotype variation - a serious problem
The first great problem was to isolate rotaviruses in tissue culture to develop less
powerful strains for use as a live oral vaccine. This has now been done. However, at least
four serotypes exist which can be distinguished from each other by specific antibody. Will
infection by one serotype provide immunity against infection by a different serotype?
Nobody yet knows the answer to this. Dr Ruth Bishops's (2) group (see="dd14.htm">DD14)
recently found that rotavirus infection of newborns did not protect them against
re-infection later on, although it appeared to reduce the severity of subsequent
infections. Thus a vaccine, even if it did not altogether prevent the disease, might still
save lives! Potential of new techniques
The techniques of genetic engineering open up new possibilities for making vaccines.
Rotavirus antigen could be implanted in common bacteria which normally colonize the small
bowel and they would reproduce the antigen and in this way immunize the patient.
Alternatively, the strain of typhoid bacillus, Ty21a, used in the new anti-typhoid vaccine
(see="#page7">page 7) might carry the rotavirus antigen. The effectiveness of
such vaccines is uncertain. The technology to make the experiment does, however, now
exist. Although some animal experiments suggest that infection by one rotavirus serotype does
not give good protection against another (3), there are nevertheless hopeful prospects. If
a vaccine can contain the two main sub-groups of rotavirus, this may provide a useful
degree of protection. More information is needed about the prevalence and severity of the
different rotavirus serotypes. Cross-disciplinary research
New kinds of rotavirus have recently been identified. Two serotypes of 'standard'
piglet rotavirus are well established and these share a common group antigen with the
rotaviruses commonly found in children. Recently, two new piglet rotaviruses have been
discovered. These are quite different from the earlier piglet rotaviruses and also from
each other, with no serological cross-reaction. A vaccine prepared against one could not
be expected to protect against any of the others. Serological tests (3) indicate that most
pigs possess antibodies to these 'new' rotaviruses, so they must occur quite widely
although rarely diagnosed. Recent reports describe new human rotavirus strains in Australia, China, Brazil, France
and Britain. They are serologically distinct, cannot be detected by current ELISA tests
and are difficult to find on electron-microscopy. The best method of diagnosis so far may
be to look for double-stranded DNA in faeces. The importance of these rotaviruses is
unknown. They have not yet been cultured and there is no immediate prospect of vaccines
against them. Also, other completely new diarrhoea viruses are still being discovered (4)
in calves and it is likely similar types will be found to cause diarrhoea in humans. Rigorous testing essential
Any vaccine launched which does not significantly reduce the total of diarrhoeal
illness among young children will rapidly be discredited. The fact that there are various
rotavirus serotypes and several other diarrhoea viruses means that manufacture will be
difficult. Before a diarrhoea vaccine is marketed, fully adequate field trials must
guarantee its effectiveness and these will need to be carried out over several years
because of the variation in viruses and the periodic nature of viral diarrhoea. In the
same place there can be 'good' and 'bad' years for rotaviruses. ORT still the best bet Prevention is always better than cure, but reliable vaccination against viral diarrhoea
seems technically unlikely to become available soon. Luckily, the cheap, simple and
life-saving technique of oral rehydration deals effectively with all acute infectious
diarrhoeas, whatever their causal organism. It must be universally publicized and applied
to save still more millions of the young children at risk. Dr T. H. Flewett, Regional Virus Laboratory, East Birmingham Hospital, Birmingham,
UK.
References (1) Schoub B D et al 1982 Variance in rotavirus infection rates in different urban
population groups in South Africa. Journal of Medical Virology, 10: 171-l 79.
(2) Bishop R F et al 1983 Clinical immunity after neonatal rotavirus infection. A
prospective longitudinal study in young children. New Eng Journal Med, 309: 72-76.
(3) Gaul S K et al 1982 Antigenic relationships among some animal rotaviruses;
virus neutralization in vitro and cross-protection in piglets. Journal of Clinical
Microbiology, 16: 495.503.
(4) Woode G N et al 1982 Studies with an unclassified virus isolated from diarrheic
calves. Vet Microbial., 7: 221- 240.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 16 February 1984
3 Page 4 5
| Measles immunization in diarrhoeal disease control |
Priority intervention?
M. and V. I. Mathan consider
whether measles immunization should be a priority in diarrhoeal disease control. In 1961, an epidemic caused by Salmonella infection occurred in a village with a
population of 527, close to Vellore in Southern India. There were 74 cases of acute
diarrhoea. More than half the patients were children less than five years old and 17 of
them had died by the time the field team reached the village. About a month before the
diarrhoea epidemic there was an epidemic of measles in the same village. Fifteen of the 17
children with diarrhoea who died, mostly due to dehydration and electrolyte imbalance, had
had measles four to six weeks before the diarrhoeal infection. Measles and diarrhoea together often fatal A prospective detailed study, in which 5,775 children in 12 villages in Bangladesh were
observed for a year, showed that measles and diarrhoea appeared to interact
synergistically* to increase mortality and the irreversible effects of nutritional
deprivation (1). Thirty-four per cent of diarrhoeal deaths were measles-associated.
Measles was the single most important cause of death during the period and diarrhoea or
dysentery was the most common complication of fatal measles cases. For every 100 children below five years of age there are about 240 episodes of
diarrhoea each year, and it is estimated that 2.1 to 5.2 per cent of such episodes are
measles-associated (2). In contrast to the average diarrhoea mortality rate of 1.4 per
cent, five to 29 per cent of young children with measles-associated diarrhoea die.
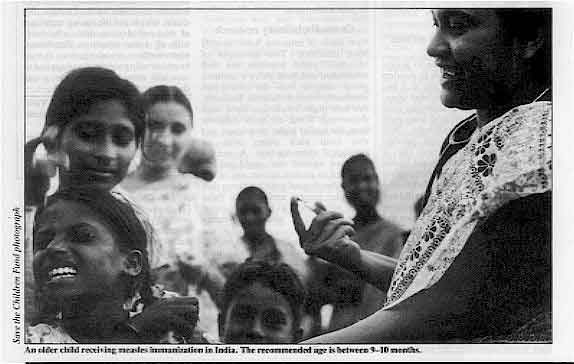 |
An older child receiving measles immunization in India.
The recommended age is between 9-10 months.
|
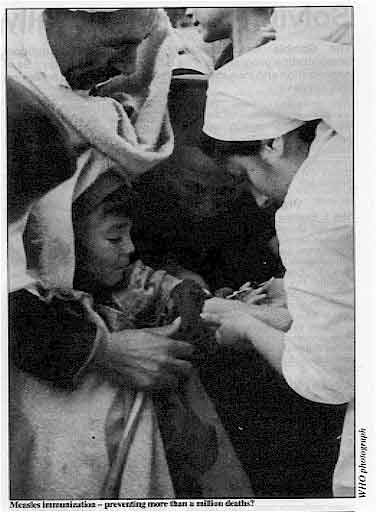
Preventing more than 1 million deaths
An effective vaccine for immunization against measles has been available for some time
and measles has almost been eradicated in several developed countries. Should measles
immunization be a major priority in the control of diarrhoeal diseases? It has been
estimated (2) that between 6.4 and 25.6 per cent of diarrhoea deaths could be prevented by
measles immunization. Assuming five million deaths each year due to diarrhoea among
preschool children in the developing world, this estimate suggests that between 60,000 to
1¼ million diarrhoea deaths a year could be prevented by an effective measles
immunization campaign. Clinical experience suggests that the cases that would benefit most
from this are the children who develop severe diarrhoea and, possibly, diarrhoea
associated with invasive organisms.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 16 February 1984
4 Page 5 6
| Measles immunization in diarrhoeal disease control |
Cost-effectiveness
A good deal of the limited funds available in the third world for the prevention
and control of diarrhoea is now spent on oral rehydration, with significant beneficial
effects. To justify using some of these funds or to find extra funds for measles
immunization as part of diarrhoeal disease control, the cost-effectiveness of such an
approach needs to be carefully assessed. There is very little available in the way of hard
data which directly estimates the effect of measles immunization on the incidence of acute
diarrhoea and of severe diarrhoea leading to death. The cost of measles immunization has
been variously estimated from US$ 2 to 15 per head, much of which will be spent in getting
properly designed delivery systems in place and working successfully. Well-controlled
studies of the cost-effectiveness of measles vaccination as a factor in the control of
diarrhoea in selected population groups are urgently needed. Simple one year study
|
Measles immunization - preventing more than a million deaths?
A quick answer could come from a simple study in a population of three to five thousand
children below the age of three years. A preliminary census survey will identify the
children who have either already had measles or who have received measles immunization.
The children will be followed up for a year, using minimally trained volunteers recruited
from the community under the supervision of one or two public health nurses. At the end of
the year, data on the incidence of new cases of measles, the incidence of acute diarrhoeal
diseases, the number of severe diarrhoeal cases and of deaths would be available. Using
the initial survey data, it should then be possible to show whether immunity to measles is
a significant factor in the mortality and morbidity. The cost of measles immunization can
be worked out by a pilot study at the end of the year of surveillance in the same
population.
|
 |
Useful extra weapon at small cost
A major constraint for the control of diarrhoeal diseases among children in developing
countries is the prohibitive cost, if a meaningful number of individuals are to be
covered. This is because the prevention of most episodes of diarrhoeal disease depends on
factors such as improved sanitation and water supplies, better nutrition and extensive
health education, most of which are interventions based on socio-economic progress. Most
clinicians who have experience with acute diarrhoea in developing countries feel that
measles immunization would be a useful immediate weapon at a comparatively trivial cost, a
feeling justified by (as yet) theoretical calculations. Some urgent but well-controlled
field trials are obviously essential to determine cost-benefits, which could then present
the policy makers with the possibility that 60,000 to 1¼ million deaths associated with
diarrhoea in the vulnerable age groups can be prevented. M. and V. I. Mathan, the Wellcome Research Unit, Christian Medical College Hospital,
Vellore, 632 004, India. (1) Koster F T et al 1981. Bulletin of the World Health Organization, 59: 901- 908.
(2) Feachem R G and Koblinsky M A 1983. Bulletin of the World Health Organization,
61: 641-652. * Synergistically - acting together, each making the other more powerful.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 16 February 1984
5 Page 6 7
Solving problems locally The Gambia has effectively implemented a
national immunization programme. Phil Gowers looks at the key
role of organization and management at community level in achieving this success. Even the best planned national immunization programmes can fail because of poor
management at community level. These are some key factors that contribute to an effective
programme: Organization
Step 1: Examine the objectives of the plan and the population you
serve. What is needed? Look for underserved areas. Calculate the number of immunizations
to be given. Step 2: Examine your resources carefully. Pay particular attention to
transport, refrigerators, deep freezes, injection and sterilization equipment. Step 3: What tasks must be carried out to achieve your
objectives? The main areas of concern are the systems which ensure that your staff
have done what is necessary to do the job properly. For example: A. COLD CHAIN
- Ordering replacements - how do you order replacement refrigerators? Does
the system work? If not, why not?
- Spare parts - are these available and does someone know how to repair your
equipment? If not, train one or two team members and arrange for the supply of tools and
spare parts. You should also have at least one, and preferably more, spare unused
refrigerators.
- Fuel supplies - particularly kerosene, must be well organized. There must
be a system for supply all the way to the clinics and an adequate reserve which will last
while the request for replenishment is being processed.
- Installation - someone, probably your repair man, will need to check the
siting of each refrigerator.
- Monitoring - someone at each clinic will need to be responsible for
checking the temperature at least once a day. A chart should be hung on the door of the
refrigerator.
B. VACCINES
- Storage - different vaccines have different storage requirements.
Checklists on correct storage procedures will be necessary for each vaccine. A member of
the team must be responsible for storage and checking when vaccines are going out of date.
The same person should fill in the report forms and vaccine requests.
- Receipt - the person responsible for storage must also sign for all
arriving vaccine and enter it into the stocks.
- Monitoring - forms will be needed to record vaccine used and people
immunized. The forms should be simple to use.
C. INJECTION EQUIPMENT
- What is needed - what size of syringes and needles are needed and
in what quantities? What method of sterilization will be used and what equipment needed?
It is preferable to have enough syringes and needles sterilized to complete a whole
clinic. Therefore the capacity of your method of sterilization is important - especially
where there is no electricity. It may be necessary to use wood fires or kerosene stoves.
If stoves are used, people must be trained to use and maintain them correctly. Your repair
man will need the tools, spare parts and skills to repair the stoves.
- Supply - as with vaccines, look at the system of ordering, receipt and
storage of equipment.
D. TRAINING
- Trainers - who is going to do the training and how? I think training
should be carried out by your supervisors. The method should be based on teaching the
tasks. The training modules produced by the WHO Expanded Programme on Immunization are an
excellent aid (1).
- Supervisors - the trainers/supervisors must be trained themselves.
- Method - the system of training should be carefully designed. One way is
to hold a 'main' training session of, say, a week for each centre and also have continuous
training for supervisors when they visit centres.
Management District Medical Officer (DMO)
The DMO will probably have overall responsibility but also has many other jobs to do.
At community level, shared management where everyone takes some responsibility and which
therefore leads to decisions everyone understands may be best. One way of achieving this
is to have the staff of each immunization unit meeting together as a team. Encourage them
to identify and resolve local problems locally. The DMO must visit each of these teams a
few times each year. Supervisor
The immunization programme will need special supervision because of the different
components involved. Someone should be trained as a supervisor and visit several units
once every six weeks or so to look at the quality of the tasks being performed (2).
By monitoring the process rather than simply the work done, the supervisor should be able
to help and support the staff in their work. Supervision involves working along with
others rather than just inspecting and instructing. Supervisors will need to be taught how
to take on this role. Phil Gowers (recently Medical Officer of Health, The Gambia), c/o London School of
Hygiene and Tropical Medicine, Keppel Street, London WC1, UK.
(1) EPI Training Modules - for information contact the Expanded Programme on
Immunization, WHO, 1211 Geneva 27, Switzerland.
(2) Fitzgerald S and Gowers P 1983 Blueprint for Success: The Gambian Immunization
Programme. World Health Forum, Vol 4, pp 79-82. Further reading See AHRTAG's two books - How to look after a refrigerator and How to look
after a health centre store (mentioned on="#page8">page 8 of this issue).
|
|
DDOnline
Diarrhoea Dialogue Online Issue 16 February 1984
6 Page 7 8
Outlook for the future
Mike Levine and others describe field trials of a new
oral vaccine in Chile and Egypt. Typhoid fever is still an important problem in many less-developed areas of the world.
Injectable anti-typhoid vaccines have long been available and provide 70 to 90 per cent
protection for up to 7 years. Because they tend to cause fever, pain and swelling at the
injection site, and a general feeling of being unwell in about one in four vaccines, these
vaccines are poor public health tools. Similar vaccines given by mouth do not cause these
unpleasant reactions. However, they give little or no protection this way against typhoid
fever, even in multiple doses. A potentially major breakthrough has been the development
by Germainier and co-workers of a new strain of typhoid bacillus, Ty21a, suitable for use
as a live oral vaccine (1). First evaluations
Initial evaluation in North American volunteers produced no adverse reactions and the
live Ty21a freeze-dried vaccine was shown to be both genetically stable and effective. The
first field trial was carried out among young Egyptian schoolchildren, who were given 1 gm
of NaHCO3 (sodium bicarbonate) to neutralize stomach acid before swallowing each of the
three doses of the reconstituted vaccine. Three years of surveillance showed 96 per cent
vaccine efficacy* (2). Field trials in Chile
With these encouraging results from Egypt, further field trials in Chile are taking
place with the following aims:
- to determine the efficacy of Ty21a given in a new form of enteric-coated capsules**
- to evaluate the efficacy of fewer vaccine doses
- to assess the vaccine's efficacy in an area where typhoid infection is particularly
common and lethal.
|
Taking live oral typhoid vaccine in the Chilean field trial.
During the first 18 months of surveillance, beginning in May and June 1982, there have
been unexpected variations in vaccine efficacy among the initial group of 90,000
schoolchildren. It is not yet clear whether these are due to the different formulation,
the different dosage schedules or the much higher force of typhoid infection that exists
in Chile as compared with Egypt.
|
 |
Sorting out the variables
From July to September 1983, in an attempt to resolve the relative importance of the
different variables, 150,000 Santiago schoolchildren were randomly allocated to one of
five groups: Group 1 - Children were given three doses of Ty21a vaccine in enteric-coated
capsules within one week. Group 2 - Children were given three doses of vaccine with NaHCO3 within one
week, both substances being contained in easily soluble gelatin capsules. Group 3 - Children were given three doses of vaccine in enteric-coated capsules
as in Group 1, but the doses were each separated by an interval of three weeks. Group 4 - Children were given vaccine and NaHCO3, in gelatin capsules as. in
Group 2, but the doses were each separated by an interval of three weeks. Group 5 - Children received three doses of placebo*** Doses of vaccine, irrespective of formulation or schedule, were intended to deliver 1
to 3 thousand million live organisms per dose. Vaccinations were well tolerated and
intensive epidemiological surveillance of the 150 thousand children is continuing. Outlook for the future
In addition to Ty21a, other candidates for new anti-typhoid vaccines are already being
investigated. The outlook for improved typhoid vaccines is therefore reassuring and the
results from the extensive field trials in Chile are awaited with considerable interest. Dr Myron M Levine, Dr Robert E Black and Dr Catterine Ferreccio, Center for Vaccine
Development, University of Maryland School of Medicine, Baltimore. (1) Germainier R and Furer E 1975
Isolation and characterization of GalE mutant Ty21a of S. typhi: a candidate strain for
live, oral typhoid vaccine. Journal of Infectious Diseases, Vol 131, pp 443-558.
(2) Wahdan M et al 1982
A controlled field trial of live S. Typhi strain Ty21a oral vaccine against typhoid: three
year results. Journal of Infectious Diseases, Vol 145, pp 292-295. For further references, write to Diarrhoea Dialogue. Authors' note
The Chilean field trials represent a collaborative effort on the part of the
Chilean Ministry of Health, the Center for Vaccine Development of the University of
Maryland School of Medicine, the Swiss Serum and Vaccine Institute, the World Health
Organisation, the Pan American Health Organisation and the Walter Reed Army Institute of
Research. * Vaccine efficacy = degree of protection produced in a group who have
been immunized compared with a similar unimmunized group.
** This special capsule covering resists acid digestion in the stomach and protects the
live organisms for release when the capsules reach the more favourable environment of the
small intestine. Such capsules would be more practical since treatment beforehand with
NaHCO3 would no longer be necessary.
*** A placebo is an inactive substance exactly similar in appearance to the active
substance being tested.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 16 February 1984
7 Page 8
Attitudes, beliefs and practices
We are working in one of the Rural Health Service Projects, undertaken by K E M
Hospital, Pune. For the last two years we have been involved in the programme of Oral
Rehydration Therapy (ORT) among the rural communities near Pune. We made some observations
on attitudes, belief and practices in relevance to the acceptance of ORT. We are
interested in fact to communicate this observation to those who are working in the field
of ORT. We would, therefore, appreciate it if you could consider our material experience
for publication in Diarrhoea Dialogue. Dr L. D. Puranik and Dr N. R. Chaudhari, King Edward Memorial Hospital, Sardar
Mudliar Road, Rasta Peth, Pune 411011, India.
These are some of the main observations made by the King Edward Memorial Hospital Team: "Village women had many different beliefs, attitudes and practices about the
treatment of diarrhoea. These differed according to the location of the village. In
communities situated close to main roads (and urban influence) women believe strongly that
only injections can relieve diarrhoea. This is a result of their constant exposure to
private medical practitioners who give injections frequently no matter what the illness.
Also, women in these areas only consult doctors when the child has become seriously ill. In more isolated areas, village women use herbal home remedies - not all of which
are helpful. For example, one remedy 'Dikamali' is mixed with sugar and used for massaging
the gums of children suffering from what mothers call 'teething diarrhoea'. This harmful
practice is thought to make the gums stronger and teething easier so that the diarrhoea
can then be controlled. Nevertheless, with continuous health education and demonstrations of how to use
ORT, over 80 per cent of rural women (especially those in more isolated communities) are
now using ORT when their children have diarrhoea. A great deal remains to be done,
however, in convincing mothers living in peri-urban communities about the value of
ORT."
Honey in ORT
Many thanks for the issue of Diarrhoea Dialogue which I got yesterday. They are
useful indeed. I do hope you will be able to send me copies of the next issues -15 of
each, so that I can forward them to our Health Units. We are now entering the hot season and so we will get more and more children with
diarrhoea. We are trying our best teaching mothers and health workers about oral
rehydration which is proved to be so useful in many cases. We have great problems with
water, being in the semi desert land of Northern Kenya. We also lack sugar but there is
honey locally made - so it can help! Our Samburu mothers are very clever and willing to learn as they love their children so
much! Sr Rosita Perino, Archer's Post C. M., P. O. Box 43, Isiolo, Kenya.
Stopping the leak In="dd08.htm">issue 8 you said that "stopping the leak
is wrong". It is a pity that the concept in Egypt is to stop the leak. Most of the
pediatricians here give combinations of antimicrobials and anti-diarrhoeals to their
patients. As a senior house officer of paediatrics, I find infants are usually brought in
to the hospital severely dehydrated after being given several prescriptions with these
combinations. - Before teaching mothers in Egypt, doctors should agree that it is dehydration that is
fatal and not the diarrhoea itself. Dr Bassma Nazmy, 10 Abou-El Karamat Street, Agouza, Guiza, Egypt.
Distributing ORS This refers to your "Meeting the demand" note in the August 1983 issue of Diarrhoea
Dialogue. Maybe the producers of "fizzy drinks and cigarettes" could be asked to help
in the distribution of ORS as part of their contribution to Health for All by the Year
2000? Dr Eilif Liisberg, Public Health Administrator, Division of Family Health, WHO, 1211
Geneva 27, Switzerland.
Practical books This issue of DD considers the interaction between measles and diarrhoea and the
importance of measles immunization. Effective immunization programmes depend on supplies
and efficient management at community level and proper maintenance of equipment and
supplies. The Appropriate Health Resources and Technologies Action Group (AHRTAG) has
published two books which deal with these important topics How to look after a
refrigerator and How to look after a health centre store. Both publications are
clearly laid out with many illustrations. They can be used by individuals or as the basis
for training a team in a health centre. Both books can be ordered from Teaching Aids at Low Cost (TALC), P. O. Box 49, St
Albans, Herts, AL1 4AX, UK. Price: How to look after a refrigerator £2.00 (plus p & p*) How to look after a health centre store £3.00 (plus p & p*) *Postage and packing rates
- Air speeded post - add on 30% of the total cost of the books. (Minimum postage and
packing is £1.50)
- Please send International Money Orders/cheques in £ sterling only.
|

Scientific editors Dr Katherine Elliott and Dr William Cutting
Executive editor Denise Ayres Editorial advisory group
Professor David Candy (UK)
Dr I Dogramaci (Turkey)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhorn (USA)
Dr D Mahalanabis (India)
Professor Leonardo Mata (Costa Rica)
Dr Mujibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Professor Andrew Tomkins (UK)
Dr Paul Vesin (France)
Dr M K Were (Kenya) With support from WHO, UNICEF and SIDA
|
Issue no. 16 February 1984
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 August, 2019
|






