|
| |
Issue no. 21 - June 1985
pdf
 version of this
Issue version of this
Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
updated: 23 April, 2014
Pages 1-8 Dialogue on Diarrhoea Online Issue 21 - June
1985
|
DDOnline
Dialogue on Diarrhoea Online Issue 21 June
1985  Page 1 2
Page 1 2
Blindness linked with diarrhoea
Nutritional blindness, caused by severe vitamin A deficiency, occurs in deprived areas
where diarrhoea is common among children. This association is not a chance happening. It
now seems that lack of sufficient vitamin A in their diet puts millions of children at
risk, not only of blindness, but also of getting diarrhoeal and other infections. At the
same time repeated attacks of diarrhoea may bring about the final eye damage which
destroys sight. Our main article describes this link and the need to do more for a child
than just treat the immediate illness. Ways are suggested on="#page7">page seven
for families to increase the vitamin A content of their children's food. Adults also at risk In many tropical countries a surprisingly large number of adults develop cataract and
become blind (see="#page2">page two). Dehydration from severe diarrhoea,
combined with malnutrition, is possibly the cause. Keeping the target in sight Although this issue focuses on a specific aspect, the overall problem of diarrhoeal
disease remains undiminished and is a major hazard in refugee situations (see="#page3">page three). Dehydration is the dangerous factor: oral rehydration
therapy (ORT) is the correct response. The rest of this page shows how one country is
making a nationwide effort to get the ORT message across. K.M.E. and W.A.M.C.
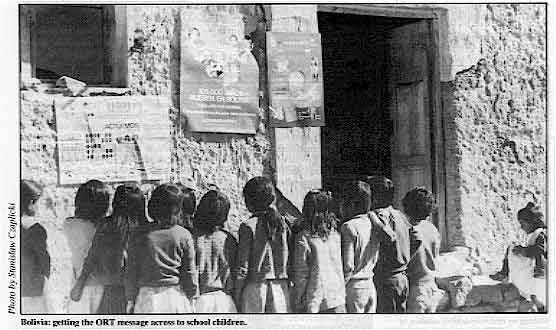
Bolivia: getting the ORT message across to school children.
|
In this issue . . .
- Practical advice on sources of vitamin A
- Diarrhoea and refugee communities
- The link between diarrhoea and blindness
|
|
DDOnline
Dialogue on Diarrhoea Online Issue 21 June
1985 1 Page 2 3
WHO booklet: training health workers Treatment and prevention of acute diarrhoea: guidelines for the trainers of
health workers.
|
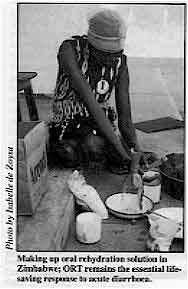
Making up oral rehydration solution in Zimbabwe; ORT remains
the essential life-saving response to acute diarrhoea.
This booklet from WHO is aimed primarily at the trainers of middle-level health
workers, to help them present oral rehydration therapy (ORT) in training courses. There is
particular emphasis on the use of ORT for children. Easy-to-follow charts summarize the
management of diarrhoea and indicate the signs and symptoms that the health worker should
look for in assessing the patient and determining treatment. The importance of good
domestic hygiene and appropriate child-care practices in preventing diarrhoea is stressed.
Single copies of the booklet are available free to DD readers from the Diarrhoeal
Diseases Control Programme, World Health Organization, 1211 Geneva 27, Switzerland.
|
 |
Book review Microbial toxins and diarrhoeal disease. Ciba Foundation symposium No 112, 1985.
Pitman Publishing Ltd., 128 Long Acre, London WC2E 9AN. Price: £27.95.
The book
is an interdisciplinary review of the diverse mechanisms whereby both new and previously
known microbial toxins disrupt the normal functioning of the intestine and produce
disease. New research findings should facilitate future 'taking science where the
diarrhoea is'(1). Oral rehydration meanwhile remains the important life-saving response to
acute diarrhoea in all circumstances. 1. Rohde J E and Northrup R, 1976 Ciba Foundation symposium No 42. 'Acute Diarrhoea
in Childhood'.
|
Diarrhoea and cataract Five years ago, the suggestion that severe diarrhoea might be partly responsible for
the high prevalence of cataract in many developing countries was first put forward. (The
role of diarrhoea had not been discussed by scientists working on cataract for over fifty
years and seemed equally new to diarrhoeal experts although old text books of tropical
medicine refer to temporary changes in the lens during cholera.) Since then several
laboratory studies have been undertaken to investigate this link (1). The hypothesis was that cataract could be caused by four features associated with
diarrhoea acting together: malnutrition; acidaemia - a condition of decreased alkalinity
of the blood; osmotic stress; and high levels of urea. The laboratory studies showed that
cyanate - a product of urea - could produce many of the changes seen in human cataract. An epidemiological survey of cataract in Raipur, India, has provided powerful support
for the diarrhoeal hypothesis of cataract. Subjects who reported 'life-threatening
diarrhoea' occurring at any time had a six-fold increase in the risk of cataract (2). The
survey concluded that 36 per cent of the cases of cataract in the area could be related to
earlier exposure to diarrhoea. There are five million people blind due to cataract in
India. If the Raipur figures could be applied to the whole country, diarrhoea might be
responsible for the blindness of two million Indian people. These findings add another
dimension to the importance of preventing diarrhoea or, second-best, preventing the
associated dehydration. Dr J J Harding, Nuffield Laboratory of Ophthalmology, Walton Street, Oxford OX2
6AW, U.K. (1) Harding and Rixon, 1980, Exp. Eye Res. 31, 567-571. Beswick and Harding, 1984,
Biochem. Journal, 223,221- 227.
(2) Minassian, Mehra and Jones, 1984, Lancet, 1, 751-753.
|
ICORT II Following the success of the International Conference on Oral Rehydration Therapy
(ICORT) in 1983, a second conference is to be held in Washington D. C. from 10-13 December
1985. ICORT II is sponsored by the U. S. Agency for International Development (AID) in
co-operation with UNICEF, UNDP, the World Bank, ICDDR, B and WHO, and will report on
progress and new developments in oral rehydration. Topics to be discussed include: health
personnel training; communications and social marketing; distribution and logistics - and
plenary sessions will focus on ways to prevent and control diarrhoeal disease; diarrhoea,
nutrition and other interventions; and new understanding of the diarrhoeal disease process
and new therapies. Simultaneous translation will be available in French, English, Spanish and Arabic.
There is no fee for attendance. Registration is required and early registration is
recommended. For further details about the conference and registration, please write to Ms
Linda Ladislaus, ICORT II Conference Staff, Creative Associates, Inc., 3201 New Mexico
Avenue, N. W., Suite 270, Washington D.C 20016 USA.
|
In the next issue...
DD 22 will
focus on the particular problems of diarrhoea and the newborn infant. We also hope to be
able to show you the results of the readers' photographic competition. |
|
DDOnline
Dialogue on Diarrhoea Online Issue 21 June
1985 2 Page 3 4
| Diarrhoea and refugee communities |
Permanent crisis
The use of ORT in difficult circumstances is nowhere better illustrated than in
refugee communities, where hundreds of people may need rehydration at any one time. The excessively high rates of mortality and morbidity in refugee camps not only reflect
the low health status of the people who become refugees but are also directly linked to
poor environmental and social conditions in the camps and inappropriate responses to the
problems(1). Minimum levels of health care, food, water and sanitation are all that can be
feasibly provided in the early days of a refugee camp. But if this approach is perpetuated
in more permanent refugee communities, public health problems such as diarrhoea may well
become worse there than in the areas the refugees have left. Trend towards ORT in Ethiopia
|
Poor conditions and overcrowding in refugee camps increase the
incidence of morbidity and mortality from diarrhoea.
It is not surprising that diarrhoea is one of the commonest causes of high rates of
disease and death in refugee camp (2). Reduction of transmission or incidence of infection
and disease is difficult enough in poor but stable communities. In a refugee setting,
additional obstacles can present very serious problems. Despite this, it is encouraging to
see how recent trends worldwide towards the use of oral rehydration therapy (ORT) have
been followed in refugee camps. During the last great famine in Ethiopia in 1973-74,
intravenous infusions were in common use at emergency clinics and hospitals. During the
current Ethiopian crisis, very few I.Vs are to be seen. However, the emphasis on oral
rehydration has underlined the need for regular supplies of larger sized packets of ORS
that make up several litres of solution at a time.
|
 |
Traditional practices
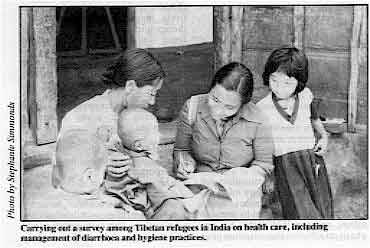 |
Carrying out a survey among Tibetan refugees in India on health
care, including management of diarrhoea and hygiene practices. Traditional good practices related to treatment of diarrhoea may sometimes mean that
dehydration is less of a problem amongst refugees than in the surrounding community. This
can be seen, for example, in the Tibetan refugee camps in India. Tibetan traditional
health care has long emphasized the need to drink extra fluids when suffering from
diarrhoea.
|
Educating refugee communities Where mothers are reluctant to give drinks to children with diarrhoea, community health
education is essential. Such education can also explain to the whole family the role of
children in the spread of diarrhoeal diseases. Children are not only the main sufferers
but also the main source of infection. If health workers in refugee communities are only
successful in getting just one message across through health education - that the stools
of small children are dangerous - and people really understand and act on this, it can be
of great importance in helping to reduce the spread of diarrhoea in the camp (3). Stephanie Simmonds, Refugee Health Group*, Evaluation and Planning Centre, London
School of Hygiene and Tropical Medicine, Keppel Street, London WC1E 7HT, U.K.
(1) Editorial, 1985. The health of refugees. The Lancet, March 23 pp 673- 674.
(2) Dick B, 1984. Diseases of refugees - causes, effects and control. Transactions
of the Royal Society of Tropical Medicine and Hygiene, 78, pp 734-741.
(3) Simmonds S et al, 1983. Refugee community health care. OUP, Oxford. N.
B. This book contains practical guidelines for the treatment and prevention of diarrhoea
in refugee communities. *WHO Collaborating Centre for the Health of Refugees.
|
|
DDOnline
Dialogue on Diarrhoea Online Issue 21 June
1985 3 Page 4 5
| Diarrhoeal diseases: combatting the long-term effects |
Treating the whole child
The immediate effects of diarrhoea are so devastating that its long-term effects
and association with related conditions are sometimes overlooked. We report on the link
between diarrhoea and nutritional blindness or xerophthalmia. Lack of sufficient vitamin A in the diet causes blindness in thousands of children in
developing countries. In Bangladesh alone, some thirty thousand children become blind
every year and at least half of them die. Throughout the world the number of children
blinded by xerophthalmia is probably half a million each year. Lack of vitamin A also puts
millions of children at greater risk from diarrhoeal, respiratory and related infections.
Blinding malnutrition results from the combined effects of poverty and ignorance. It is,
however, a problem which can be greatly reduced and, in time, eliminated. As death from
diarrhoea can be prevented with oral rehydration therapy (ORT), blindness caused by
xerophthalmia can be prevented by an increase of vitamin A in the diet. The success of
both these interventions is heavily dependent on effective community health education (seepage six). Stages in the development of xerophthalmia Xerophthalmia is caused by an extreme shortage of vitamin A in food intake. Many of
those affected die from the associated malnutrition, increased susceptibility to common
infections and a lowered immune response. Even mild degrees of vitamin A shortage can
damage the body's protective epithelial surfaces which line intestinal, respiratory and
urinary tracts as well as covering the eyes. 'Night blindness', difficulty in seeing in a
poor light, is a first sign of vitamin A deficiency. Affected children become clumsy in
the dark and, where xerophthalmia is common, communities recognize this condition and
often have a traditional name for it. Unless vitamin A intake is increased, the condition
may get worse, especially where children suffer from diarrhoea and other infections. Night blindness is followed by conjunctival xerosis; the covering of the eye becomes
dry, rough and wrinkled instead of remaining smooth and shiny. Bitot's spots can often be
seen - these are foamy patches near the lateral side of the iris, the coloured part of the
eye. The next stage is particularly serious as it affects the cornea, the clear area over
the iris through which objects are seen. It also becomes rough, and eventually opaque.
Finally, the cornea becomes soft (keratomalacia) and the eyeball may perforate. Even if
corneal ulcers heal there will be severe scars and, if the eye collapses, vision is lost.
Nevertheless, all of the early stages of eye damage described can be reversed by effective
treatment. It is always very important to remember that blindness is often precipitated by
infections - particularly diarrhoeal diseases. These rob the body of already scarce
reserves of vitamin A. Prompt and comprehensive treatment of these illnesses will save
both lives and sight (see below).
Treatment of
xerophthalmia
(W.H.O. 1982) |
| |
Vitamin A
|
|
|
200,000 IU by mouth |
|
|
200,000 IU by mouth |
- Day 14
- earlier if eyes worsen
|
200,000 IU by mouth |
| Diarrhoea and vomiting: 100,000 IU water soluble vitamin A by
intra-muscular injection if available. Under 12 months:½ the dosage |
The link with diarrhoea and measles Blindness becomes an immediate risk among ill-fed children when infections like measles
and diarrhoea occur. Measles can be prevented by immunization; and the WHO/UNICEF emphasis
on effective immunization programmes should reduce this particular danger where the
measles virus can directly attack eyes already weakened by a mild degree of
xerophthalmia.
Repeated attacks of diarrhoea are closely associated with the onset of
xerophthalmia. Diarrhoea contributes to nutritional blindness in several ways. During the disease,
food intake is limited and absorption decreased. Diarrhoea occurs more often and more
seriously in malnourished children who have very poor stores of vitamin A in the liver. A study in Bangladesh showed that at least half of the children who had serious
xerophthalmia had suffered from diarrhoea in the previous month. In Indonesia, children
with xerophthalmia were five times as likely to have had diarrhoea in the last week as
children without signs of vitamin A deficiency. Dealing with xerophthalmia Children most likely to develop xerophthalmia are those who are already malnourished
with grossly inadequate intakes of energy, protein and fats as well as of vitamin A.
However, a recent study in Indonesia showed a high frequency of vitamin A deficiency in
children who were not malnourished (1). Vitamin A deficiency is a complex problem of more
than just food intake. In the long term, better feeding of young children is the way to
control the problem (see="#page6">page six of this issue). In the short term,
regular distribution of vitamin A supplements to children-at-risk is useful and
comparatively inexpensive. The cost of a therapeutic dose of 200,000 International Units
(IU) of vitamin A is approximately two US cents and will be effective for up to four
months since vitamin A is stored in the liver. Among severely malnourished children, the
supplements need to be given more frequently, as, for example, in feeding programmes for
young victims of famines like the one affecting Africa.
|
|
DDOnline
Dialogue on Diarrhoea Online Issue 21 June
1985 4 Page 5 6
| Diarrhoeal diseases: combatting the long-term effects |
Treatment guidelines
|
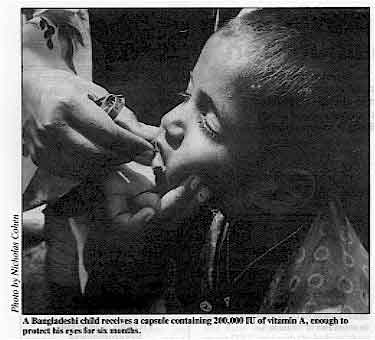
A Bangladeshi child receives a capsule containing 200,000 IU
of vitamin A, enough to protect his eyes for six months.
The following guidelines for treatment are important:
- Examine the eyes of all children with diarrhoea. In all areas where xerophthalmia is
common, be sure to see the eyes of every child who comes to a clinic. This includes those
who are crying and those who are sleeping. Too many children go blind 'behind closed
eyelids'.
|
 |
- Make sure all children with diarrhoea receive effective oral rehydration without delay.
This will promote appetite and intestinal absorption of food. Any associated respiratory
or other infections should be appropriately treated. Re-feeding should start as soon as
possible following rehydration. Breastfeeding should be encouraged and practical advice
given about improving the diet to include some vitamin A rich foods. (An earlier issue of="dd10.htm">DD, number 10, describes the work of the Children's Nutrition
Unit in Dhaka, Bangladesh, where xerophthalmia is common. Families learn how to make
better use of local food resources without having to spend more money.) Some governments
are fortifying foods with vitamin A - such as the long-standing sugar fortification
programme in Guatemala.
- If the eyes show signs of xerophthalmia, follow the WHO recommended treatment schedule (see box). All damage to the eye can be cured up to the stage of
severe corneal damage.
- All malnourished children with measles are at high risk of blindness and this can
develop within a few hours. Give vitamin A in the recommended dose unless the child has
received a large dose within the last four months.
Breastfeeding to protect sight The unborn child gets vitamin A from its mother through the placenta. If the mother's
diet is inadequate, the newborn starts life without a sufficient store of vitamin A in its
liver. Premature infants are particularly at risk and babies may even be born with -
obvious xerophthalmia. Young children cannot store much vitamin A and need to have a small
but regular supply in their diet. In those countries where vitamin A deficiency is most
common, babies depend mainly on breastmilk for their supply. The highest concentrations
occur in colostrum (the substance secreted by the breasts during the first few days after
delivery). In societies where it is not the custom to allow babies to have
colostrum, a
valuable early source of vitamin A as well as other protective substances is wasted. The
amount of vitamin A in breastmilk gradually decreases but is always higher than in cow's
milk. Breastfeeding therefore protects against xerophthalmia, although breastmilk from a
poorly nourished mother may be low in vitamin A and may also be insufficient in quantity
to prevent a degree of malnutrition. Where the average diet is known to be vitamin A
deficient, mothers can be given a megadose (200,000 IU) by mouth after delivery and this
will raise the levels of vitamin A in their milk for at least 3 months. Too much vitamin A
can, however, harm the unborn child. Doses greater than 10,000 IU should never therefore
be given to a pregnant woman, or one who is breastfeeding but who may also have an early
pregnancy. Even without vitamin A supplementation of the mother, the risk of xerophthalmia
for children under two who are not breastfed is nevertheless 6-8 times greater than for
those receiving breastmilk. Caution Infant formula foods usually contain added vitamins, including vitamin A. Dried skimmed
milk (DSM) has had the vitamin A removed in processing, along with other fat soluble
vitamins such as D and K. DSM used in nutrition feeding programmes must be fortified with
vitamin A. Always check the pack label for the vitamin A (and D) content. Many children
have been blinded through wrong use of non-fortified dried skimmed milk. Based on material provided by Nicholas Cohen, Mira Mitra, E. Leemnuis de Regt, J.
Davidson of Helen Keller International, Bangladesh, in collaboration with the Institute of
Public Health and Nutrition, Dhaka, Bangladesh. (1) Low vitamin A linked to death. Dr Alfred Sommer, John Hopkins University,
Baltimore, USA. Study reported in Science News, October 13, 1984. USAID is funding Dr Sommer at the John Hopkins University to enable him to continue his
research.
|
|
DDOnline
Dialogue on Diarrhoea Online Issue 21 June
1985 5 Page 6 7
Vitamin A: preventing blinding malnutrition
There is no real scarcity of vitamin A in many African and Asian countries.
Problems arise when fruit and vegetables containing vitamin A cannot be conserved, or when
it is not culturally acceptable for or is difficult to get children to eat vegetables. In many areas where xerophthalmia is prevalent there is an abundance of fruits and
vegetables that provide a natural source of vitamin A. These are, however, often not
eaten, especially by children, the main group who suffer from blinding malnutrition. Many
nutrition education programmes are now focusing specifically on children. School children
are an ideal target for learning the importance of fruits and vegetables to family health.
There are many ways of preparing green vegetables to make them more acceptable to children
- for example, chopped and mixed with lentils and other pulses, minced meat, stews and
soups. If children still refuse to eat greens, and the family cannot afford the animal
foods containing vitamin A (see table), carrots and coloured fruits are also useful
sources. It is important to note that vitamin A cannot be satisfactorily absorbed by the
body unless there is sufficient oil or fat in the diet.
Common sources of vitamin A |
| Ready-made sources |
Carotene sources* |
| Meat |
Green and yellow vegetables (especially dark green leaves) |
| Liver |
|
| Fish |
Red palm oil |
| Milk and dairy produce |
Yellow marrow. pumpkin and squash |
| Eggs |
Carrot, mango and papaya |
| *The body makes vitamin A from carotene in the diet. |
Conserving vegetables (containing vitamin A) out of season
|
Sun dryer for vegetables. A simple shade should be
supported over the tray to avoid loss of vitamin A. In areas where fruits and vegetables may not be available all year round, sun drying is
a useful way of preserving supplies. Perishable fruits are often lost on the way to
markets and can be transported more easily in a dried form. A simple sun dryer like the one shown in the illustration can dry up to 60 kilos of
green vegetables a day in a hot, sunny climate. A most important point is that the
vegetables must not be exposed to direct sunlight since this destroys a lot of vitamin A.
|
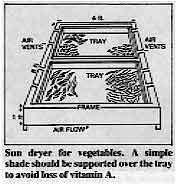 |
To avoid this, a simple shade of reeds, stretched hessian or cloth can be supported
over the drying tray. This does not interfere with the drying process as the drying is
accomplished by sun-heated air rather than by direct sunlight(1). Dried green vegetables and suitable root and fruit crops will provide concentrated
amounts of vitamin A. What is vitamin A? Vitamin A is a fat-soluble substance, retinol, found in animal foods and dairy
products. Carotene, the naturally occurring substance from which vitamin A is made either
by humans or animals, is manufactured by plants, particularly those with dark green leaves
or with reddish yellow roots or fruits. Dietary fats, pancreatic enzymes and bile salts
are all important for the absorption of both vitamin A and carotene, which are transformed
by the lining of the intestine into retinol.
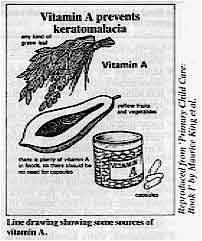 |
Vitamin A prevents keratomalacia. Line drawing showing some sources of
vitamin A. Most vitamin A is stored in the liver as retinyl palmitate. Free retinol is highly
active but toxic and it is therefore transported in the body in combination with a
retinol-binding protein. Retinol is essential for the proper functioning of the
photo-receptor cells which detect light striking the retina at the back of the eye. Hence
the night blindness in early vitamin A deficiency. It is also necessary for the production
of healthy new cells to cover the eye and line the different body systems like the gut and
respiratory tract. Severe deficiency damages the body's defence against infections. Severe
xerophthalmia and keratomalacia only occur when liver stores of vitamin A are extremely
reduced.
|
(1) Appropriate technologies for tackling malnourishment. Jim McDowell CONTACT 45,
June 1978. Further reading: Xerophthalmia Club Bulletin. Produced by Mrs A Pirie,
Nuffield Laboratory or Ophthalmology, Oxford, U. K.
|
|
DDOnline
Dialogue on Diarrhoea Online Issue 21 June
1985 6 Page 7 8
ORT in Fiji I am a medical student in Fiji, catering for about 6,300 people. The health centre
where I works is about 80-90 miles away from the nearest town and we are very fortunate
indeed that your newsletter has reached us. It helps us to refresh and modernize our ideas
as far as diarrhoeal treatment is concerned. The efficacy of ORT in this area acts as a
miracle in the treatment of diarrhoea and is very useful to combat loss of body fluids and
electrolytes. Primary Health Care seminars, village visiting and clinics contribute to the
wide acceptance of ORT in this medical area. I would like to thank you once again for the
issues we have received and hope to receive future issues. Mosese Palasklo, Tukavesi Health Centre, Bucca Bay, P. O.
Tukavesi, Fiji
Island.
Motivating the community
I am working as a sanitation co-ordinator with the Juba Water and Sanitation Programme.
We are launching a Health Education Programme and E.P.I. I make ten home visits and hold
two block meetings a month. Juba, the capital of Equatoria Region in the Sudan, with a population of 120,000
people, has poor sanitation and the programme is trying to motivate people to improve the
situation. I am a regular receiver of DD which I find informative and educational.
As the main language spoken at home here is Arabic, I am asking you to mail to me at least
ten copies of DD quarterly so that I can distribute it during my home visits. Simon Ladu Atunya, Sanitation Co-ordinator, Juba Water and Sanitation Programme,
Directorate of Housing and Construction, Juba, c/o OXFAM - SUDAN, PO Box 40680, Nairobi,
Kenya.
Importance of DD I am working as an endemic diseases control unit assistant in the Ministry of Health,
Bo, Sierra Leone, West Africa. As a field worker the few copies of Diarrhoea Dialogue sent
to me have been of great help to me since I am now using it to advise our people about the
causes and prevention of diarrhoea. With the help of Diarrhoea Dialogue I
have been explaining to people that feeding bottles that most mothers use for feeding
their children are one of the main causes of diarrhoea. ORT has also been very quick and
economical in reviving a diarrhoea patient. I extend my greatest thanks to the producers of the Diarrhoea Dialogue who
are going all out to save lives of millions of people. I may be very happy if more copies
are sent to me and if possible other materials. I have some friends who are working with
me and may like to get some copies through me. Aiah Alpha, E. D. C. Unit Assistant, Ministry of Health, Bo, Sierra Leone, West
Africa.
Farsi edition I was really quite enthralled receiving="dd19.htm">Diarrhoea Dialogue, issue
19. I am an Indian GP working in Iran for the past four years with opportunities to
visit villages where 'Dharmanghas' (dispensaries) are located and come into contact with
the local people almost every day in the course of my routine duties. I find these people
a little recalcitrant about ORT, and with the little working knowledge of Farsi (the
Persian language) I have, I am able to convey the advantages of ORT over conventional
therapy, Though the slides along with the commentary which I got taped in Farsi language
have been helpful - I got the slide set through the agency TALC - I would appreciate it if
you can expand the readership of Diarrhoea Dialogue to Farsi too; it would
certainly be of immense help in a country like this - with dedicated workers in the field,
who are aware of diarrhoea and its consequences in children. Dr K. S. Narayana, Aligoudarz, Lorestan, Iran.
Diarrhoea in refugee communities
|
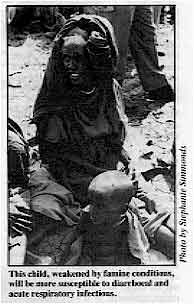
This child, weakened by famine conditions, will be more
susceptible to diarrhoeal and acute respiratory infections.
I am a Somali general practitioner and work for the refugee health unit of the Ministry
of Health in Somalia. Diarrhoea and acute respiratory infections are two major health
problems in the refugee camps. We have developed plans to try to reduce mortality. We
rarely get an opportunity to keep in touch with what is going on outside. Sometimes our
head office in Mogadishu sends copies of Diarrhoea Dialogue. Recently, while I was
preparing some materials for the camp medical teams, I received issue
19 of DD. This gave me some very useful information for the materials I was
developing on oral rehydration therapy. Dr Mohamed Ali Farah, Regional Director of Refugee Health, Unit North West Region,
Hargeisa, Somalia. Editors note: see="#page3">page three of this issue.
|
 |
Using the DD index The index of material from issues 1-19 in issue 20 of DD has proved very useful
indeed. Part of my work here in Kabwe involves compiling a resource library of health
education materials. Diarrhoea Dialogue being one such reference. Thanking
you for your kind assistance. Margaret O'Meara, Health Education Unit, Kabwe Urban District Council, P. O. Box
80424, Kabwe, Zambia.
Health basics I would like to thank you for the section showing what to do when dehydration occurs
and the plan for severe dehydration, in="dd19.htm">DD19 on ORT: the
life-saving solution. The issue covers most of the things we require to do to prevent and
treat dehydration. I have used it to teach my nurses, aid post orderlies and parents in
the wards how to assess the degree of dehydration and what to do for severe dehydration. I
treat more diarrhoea cases in my Health Centre and at my MCH clinic patrols in the
villages. Diarrhoea Dialogue helps me a lot in the management of diarrhoea. Mr Nang Bomai, Health Extension Officer, Kilau Rural Health Centre, Simbu Province,
Papua New Guinea.
|
|
DDOnline
Dialogue on Diarrhoea Online Issue 21 June
1985 7 Page 8
Ways to promote ORT in India While working as the Senior Resident Medical Officer in the Paediatrics Department of
one of the busy hospitals of Bombay, I found the following points worth mentioning:
- About 50% of indoor admissions and 30% of outdoor patients are suffering from
diarrhoea and/or malnutrition. But our patients are not yet aware of oral rehydration
therapy and still insist on drugs and injections for diarrhoea treatment. It is very
difficult to change their minds in spite of a lot of explaining and there is always a
shortage of time in a busy outpatients department.
- I have found that many senior paediatricians and private practitioners are still
focusing their attention on antibiotics and antidiarrhoeals as part of their treatment of
diarrhoea. It is these people who have influence over patients and community. Unless
senior colleagues start changing their attitudes, patients won't have faith in our junior
doctors. Your newsletter is focusing attention on teaching health workers, but I think
that doctors in India need equally to learn about ORT. Some of them even discourage
breastfeeding and food and go on prescribing useless and harmful drugs (though patients
here are very fond of drugs).
- I think all the junior doctors including medical students should be taught from the
beginning about ORT and other aspects of diarrhoea. All the senior doctors and other
paramedical workers should be kept in touch with recent advances in management of
diarrhoea through lectures, seminars etc. Magazines like DD can do much in
this regard.
- I have been much influenced by diarrhoea control programmes in other developing
countries. Surprisingly I have not heard much regarding the same in our country. Though we
have been using ORT since a few years ago I think people should be made aware of the use
of ORT through widespread use of media like TV and radio.
Lastly I must congratulate you on your efforts towards controlling diarrhoea, and use
of ORT. Dr M B Bhagat, 16 Jawahar Nagar, S V Road, Goregaon (West) Bombay 400 062, India.
Reducing nausea and vomiting Reading your December 1984 issue my attention was drawn to the="su19.htm">insert
called Health Basics and the paragraph headed 'What should be done if the child vomits'.
You have suggested that the child should be given regular small sips of fluid. I fully
agree, but many small children continue to be nauseated and continue to vomit when given
small sips of fluid. It is possible to further reduce nausea and vomiting by getting the
child or adult to suck the ORT through a straw. If the patient is still nauseated and continues to vomit or has a diminishing level of
consciousness, quite large amounts of fluid can be taken orally if they are given the
opportunity to suck a wet or damp cloth. This cloth may be arranged in the form of a wick
from the reservoir of ORT. Nausea or vomiting is usually given as the reason why a
particular patient was not given ORT and was either not rehydrated or resort was taken to
intravenous fluids with all the consequent problems of expense, short supply and the
requirement of a greater level of expertise to do it properly. Martin Schweiger, Specialist in Community Medicine, Leeds Eastern Health Authority,
St Mary's House, St Mary's Road, Leeds LS7 3JX, U. K.
Diarrhoea and malnutrition I'm the medical superintendent of Matany Hospital, a missionary hospital in Central
Karamoja. I'm in charge of the Primary Health Care plan of the hospital. Karamoja is a
very dry area and the problem of diarrhoea and malnutrition connected in a complex is the
most important problem of PHC in our area. I work strictly with our ten health educators.
Every number of Diarrhoea Dialogue is read by them and me and discussed together.
Sometimes we look to the past numbers but unfortunately we don't have some issues. These
are numbers 1,5, 7,9, 11 and 12. I'd like it if you could supply us with these past
issues. Dario Zanon, Matanay Hospital, P. O. Box 46, Moroto, Karamoja, Uganda.
Writing a proposal I want to register my appreciation of issue 20. I am a third year student in the
Department of Geography and Environmental Studies. Issue 20 coincided with the time I had
to submit a research proposal for my final year dissertation. I had selected a topic on
medical geography; a case study on the volume of water borne diseases in the inhabited
islands of the Great Scarcies River, but my problem was how to come up with a concise
proposal. The article on="dd20.htm#page6">page six of issue 20 on How to
write a proposal was so saliently, excellently and simply put that I immediately
discarded all the previous literature I had consulted in preference to DD. Many
thanks and please include my name on your mailing list. Patrick A S Kamora, Njala University College, P. M. B. Freetown, Sierra Leone.
|

Scientific editors Dr Katherine Elliott and Dr William Cutting
Executive editor Denise Ayres
Editorial assistant Kathy Attawell
Editorial advisory group
Professor David Candy (UK)
Dr I Dogramaci (Turkey)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhorn (USA)
Professor Leonardo Mata (Costa Rica)
Dr Mujibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Professor Andrew Tomkins (UK)
Dr Paul Vesin (France)
Dr M K Were (Kenya) With support from AID (USA), UNICEF and WHO
|
Issue no. 21 June 1985
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 April, 2014
updated: 23 April, 2014
|






