|
| |
Issue no. 4 - February 1981
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-8
Diarrhoea Dialogue Online Issue 4 -
February 1981
|
DDOnline
Diarrhoea Dialogue Online Issue 4 February 1981
 Page 1 2
Page 1 2
A unique chance
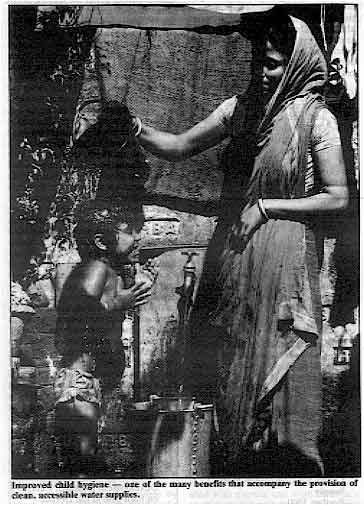 |
Improved child hygiene - one of the many benefits that
accompany the provision of clean, accessible water supplies.
The International Drinking Water Supply and Sanitation Decade launched last November
could improve the quality of human life throughout the world more than any previous
initiative by the United Nations. The benefits of clean, accessible water are
considerable. Life may change dramatically for many women in the developing world who
often spend hours every day fetching the minimum of water necessary for their families'
survival. And, because healthy people are productive people, cleaner drinking water can
have resounding economic consequences. But the Decade's greatest potential is the chance it offers to save the lives of so
many children in the developing world. Today, 800 million people live in absolute poverty
- their children are their only hope. If, during the next ten years significantly fewer
children die and productivity is increased through better health, we may have an entry
point to break the poverty cycle.
|
The supplying of clean drinking water must be accompanied by the provision of
sanitation and by education about hygiene. The high cost will mostly have to be borne by
the developing countries. However, the Water Decade offers a unique opportunity for
cooperation between the leadership of both developed and developing nations. The need for
water, coupled with the desire to stop children dying, is a topic about which complete
agreement ought to be possible. Peter Bourne, Assistant Secretary General, UNDP, and Coordinator, International
Drinking Water Supply and Sanitation Decade. World Bank photo by Ray Witlin
In this issue . . .
- Richard Feachem discusses priorities for diarrhoeal disease control.
- Anne Whyte looks at community participation, water and health.
- John Cuthbert reviews hand pumps.
|
|
|
DDOnline
Diarrhoea Dialogue Online Issue 4 February 1981
1 Page 2 3
Guest editor
Our guest editor for this issue of Diarrhoea Dialogue is Richard
Feachem, Senior
Lecturer in Tropical Public Health Engineering at the Ross Institute of Tropical Hygiene,
London School of Hygiene and Tropical Medicine, London, U.K. Indonesian Congress The fifth Indonesian National Congress of Paediatrics will be held in Medan, North
Sumatra from 14 to 18 June 1981. The theme of the Congress will be Optimal growth and
development for a bright future. Further information can be obtained from
Helena Siregar, Chairman, Konika-V, Department of Child Health, University of North
Sumatra, Medan, Indonesia. Linking resources to needs A recent conference organized by the National Water Council (NWC) in the United Kingdom
provided the first British follow-up to the launching of the UN Water Decade. The purpose
of the meeting was to provide information about the Decade's aims and to focus attention
on how British professionals concerned with water, and the wider public, may best
contribute skills and resources. Speakers included Peter Bourne, John Kalbermatten, Richard Feachem and representatives
from the government and non-governmental organizations (NGOs) in the U. K. The conference
was given a sharp visual reminder of the severity of water supply and sanitation problems
in many developing countries through slides and the UN film "Journey for
Survival". A major theme of the conference was the best way of linking the technology and
resources of the West to the needs of developing countries. Peter Bourne commented that
the initiative taken by the NWC provided a useful model that could be used elsewhere to
inform people about the specific needs of the Decade and to provide a channel for
technical assistance. The role of charities such as Oxfam and the Save the Children Fund
was also mentioned in this context, together with other NGOs such as the Intermediate
Technology Development Group. The importance of training at all levels both in the U. K. and in developing countries
was widely endorsed, although fears were expressed about the prohibitively high costs of
bringing students to the U.K. for courses. Several speakers emphasized that technical assistance should be provided on request
from developing countries and that programmes should focus on the needs of particular
areas, rather than "master" plans for entire regions. This led on to discussion
about health education and community participation in water and sanitation projects. There
was debate about the difficulties of continued maintenance and financing of local schemes
within the existing social and economic structures of many developing countries. The conference discussions took on more meaning the following day as water and sewage
workers in the U.K. threatened a national strike. One possible result of such action would
have been that within a few days people in London would have had to boil drinking water to
ensure its safety. An irritating necessity - but also a timely reminder of the kind of
problems that confront the UN Decade. Literature on water supply and sanitation
Some of the organizations which produce literature on water supply and sanitation are:
- Centre Panamericano de Ingenieria Sanitaria y Ciencias del Ambiente
Casilla Postal 4337
Lima 100
Peru
- Environmental Health Division
World Health Organization
1211 Geneva 27
Switzerland
- Environmental Sanitation Information Centre
Asian Institute of Technology
PO Box 2754
Bangkok
Thailand
- Intermediate Technology Publications Ltd
9 King Street
London WC2E 8HN
United Kingdom
- International Development Research Centre
PO Box 8500
Ottawa
Canada K1G 3H9
- National Environmental Engineering Research Institute
Nehru Marg
Nagpur 440020
India
- Ross Institute of Tropical Hygiene
London School of Hygiene and Tropical Medicine
Keppel Street
London WC1E 7HT
United Kingdom
- Transport, Water and Telecommunications Department
The World Bank
1818 H Street, NW
Washington DC 20433
USA
A major and important series of publications (3 books and 12 reports) is currently
being published by the World Bank and will be available during 1981.
- WHO International Reference Centre for Community Water Supply
Postbus 5500
2280 H M Rijswijk
The Netherlands
- WHO International Reference Centre for Waste Disposal
Ueberlandstrasse 133
CH-8600 Dübendorf
Switzerland
In the next issue . . .
- articles from the World Bank, WHO and the International Development Research Centre on
their role in the Decade
- reports on water and sanitation programmes in Mocambique and Nepal
- practical advice on dry latrines
- more news and letters
Diarrhoea Dialogue 5 will be available at the end of May
1981. |
|
|
DDOnline
Diarrhoea Dialogue Online Issue 4 February 1981
2 Page 3 4
| Communities. water and health |
Decisions taken by ourselves for ourselves
Attitudes to water use and sanitation remain some of the most resistant to change.
Anne Whyte explains how this can be remedied through increased
community participation in projects. In 1975, only about 20 per cent of rural people in developing countries had reasonable
access to adequate water and sanitation. Everyone can tell stories of projects that have
failed; hand pumps that break within months and remain broken for years, latrines that are
built but never used. The International Drinking Water Supply and Sanitation Decade
crystallizes an approach to development in water and sanitation that has evolved over the
past ten years. It is based on:
- more community participation
- closer links to other sectors, particularly health education and primary health care
- the development of low cost, self-reliant and self-sustaining projects.
Community participation is the most political aspect of the Decade approach because it
directly involves the relations of a national government to its people. To succeed, it
clearly needs political commitment at all levels. What is community participation? For some people community participation is an ideology of development. For others, it
is a practical means of planning and management. To supply the needs of the world's people
for water and sanitation, it may be the only means available to us. Community participation is sometimes called "popular participation",
"self-help", or "self-reliance". These are all relative measures of
how much things are being done for people by others or by people for themselves. In other
words, community participation means people are making decisions and taking responsibility
for:
- planning projects and setting goals
- implementing projects
- sharing benefits
- evaluation of projects.
Priorities
People have an opportunity to express their own needs through community participation.
Their priorities may not be for water and sanitation. Governments and development agencies
may have to respond to community priorities on the one hand, but also be prepared to
provide health education to change community views and behaviour. The role of behaviour
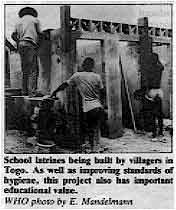 |
School latrines being built by villagers in Togo. As well
as improving standards of hygiene, this project also has important educational
value.
WHO photo by E. Mandelmann The extent and severity of diarrhoeal diseases among preschool children is related to
poor water and sanitation, malnutrition, inadequate housing and human behaviour. Mothers
prepare food with hands and water contaminated with excreta and wash children's clothes,
soiled with faeces, in streams that become the water supply for others. They may not
perceive the same differences between safe and contaminated water that we do. Biologically
"safe" well water may taste strange and be rejected for the contaminated but
familiar stream.
|
Changing attitudes
Educating people to change their behaviour in order to prevent disease is one of the
most difficult and important tasks in health education. Attitudes and behaviour related to water use and sanitation are some of the most
difficult to change. In most cultures, the way in which water is distributed and owned,
reflects the local balance of power. Water control brings political control, so that when
a new water supply is introduced, it may bring with it far-reaching social and political
changes within the community. Water sources are often social places. People meet at the stream, spring or borehole.
Carrying water can identify your status in the community. One household collects water at
the source; another lets it be seen that they send a servant or buy from a water seller.
Most water carriers are women and children. Despite the heaviness of the task, it is not
men's work. Personal hygiene practices related to water and sanitation are also difficult to
change. Defaecation habits are among our most personal ones and require a sensitive
approach to health education. It is a difficult message to get across that a mother may be
the cause of disease in her family. Health education
However, the outlook is encouraging. Health education and primary health care are being
more closely integrated with planning for water supply and sanitation, and at an earlier
stage. By focusing attention on children and the need to change their behaviour, health
education to improve parents' habits can be transmitted in an unthreatening way. A
community participation approach to health education can involve families in monitoring
disease, evaluating their own behaviour and identifying ways of improvement. Perhaps the most important message for all involved in community development is that decisions
taken by ourselves for ourselves make us more committed to making those decisions
work. That is one important hope for increasing community participation in water and
sanitation projects over the next Decade and beyond. Anne Whyte, Institute for Environmental Studies, University of Toronto, Toronto,
Canada.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 4 February 1981
3 Page 4 5
| Priorities for diarrhoeal disease control: clean water and
sanitation |
Water, excreta, behaviour and diarrhoea Improving only water quality or only latrines will have little or no effect on the
incidence of diarrhoeal disease. Richard Feachem discusses how
only an integrated control programme can be effective in the long term. Oral rehydration and other curative approaches to diarrhoea may have a great effect
upon mortality, but they cannot significantly reduce transmission or the incidence of
infection and disease. Most children may be kept alive by a comprehensive curative
programme which makes simple therapy readily available in the village, but they will
continue to be regularly reinfected. The main goal of diarrhoea programmes must therefore
be control. How is control to be achieved? There are three basic approaches:
- interrupting transmission by the improvement of water supply, excreta disposal and
hygiene
- improving the general health of children by improved nutrition and reducing the
incidence of other infections
- immunization.
In the long run control will be achieved by a combination of each of these approaches
but it is significant that, in developed countries, and in wealthy communities in
developing countries, control has been achieved by a combination of the first two alone. Rich and poor
Diarrhoeal disease is associated with poverty and with the environmental and
educational conditions that accompany poverty. In wealthy communities throughout the world
diarrhoeal disease has become a minor public health problem. If we look at Europe and
North America, for instance, some infections have become very rare (Vibrio cholerae,
Shigella species other than sonnei, Salmonella typhi and paratyphi and Entamoeba
histolytica) while other infections continue to occur but cause little disease
compared to their status in developing countries (rotaviruses, enterotoxigenic E.
coli, salmonellae, Campylobacter and Shigella sonnei). The fundamental question in diarrhoeal disease control is how may
the diarrhoea pattern of a poor community be transformed to the pattern of a wealthy
community? If this transformation requires the elimination of poverty and a
substantial improvement in incomes and educational levels, then we should not talk of
diarrhoeal disease control but focus instead on overall economic development and political
change. However, there is some evidence that diarrhoeal disease transmission in poor
communities can be reduced in the short term by improving water supply, excreta disposal
and hygiene, prior to any reduction in poverty and deprivation in the longer term. Transmission
The classical view of diarrhoeal disease transmission, derived from studies of major
urban common-source outbreaks, was that it is primarily associated with faecally
contaminated drinking water - in other words it is water-borne. This view has been
progressively modified as more and more information has come to light on the
non-water-borne transmission of diarrhoeal diseases in both endemic and epidemic
situations.
|
Pigs contaminate the pond surrounding an open, hand-dug well
in Upper Volta. There is no drainage and the water in the well will be heavily polluted.
World Bank photo by Ray Witlin It now seems very probable that, among poor people in developing countries, most of the
spread of organisms which cause diarrhoea is by faecal-oral routes that do not involve
drinking contaminated water. All the main diarrhoea-causing pathogens* are transmitted
from anus to mouth and there are many opportunities for such transmission in a poor and
crowded community. Water-borne transmission is but one special case of faecal-oral transmission and most
authorities would agree that a great deal of the transmission of rotaviruses,
shigellae,
enterotoxigenic E. coli and Entamoeba histolytica is by non-water-borne
routes. There is less agreement on the transmission of cholera. Some suggest that cholera
is largely water-borne everywhere; others that it is mainly water-borne in Bangladesh but
not necessarily elsewhere. However, a third group maintain that it is not primarily
water-borne anywhere.
|
 |
Water quality
Water-borne transmission is reduced by improving water quality. Many people drink
heavily contaminated water (containing up to 10 / 4 E. coli per 100
millilitres)
from open wells, ponds or streams. Replacing these sources by piped water or protected
wells will dramatically improve water quality and will therefore reduce water-borne
transmission. However, some studies in Bangladesh (1), Guatemala (2), Lesotho (3), the
United States of America (4) and elsewhere have found that such improvements failed to
have a marked effect on diarrhoeal disease incidence. One possible explanation for these
findings is that diarrhoeal diseases in the communities studied were mainly
non-water-borne.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 4 February 1981
4 Page 5 6
| Priorities for diarrhoeal disease control: clean water and
sanitation |
Water availability and water use If diarrhoea-causing pathogens are being transmitted by non-water-borne routes (for
instance on hands, clothes and food) it is important to improve personal and domestic
cleanliness. This is difficult, if not impossible, when the nearest water source is far
from the house and the water must be laboriously carried in small containers. It is also
difficult when there is a tap near the house which provides only an intermittent supply.
Improved personal and domestic cleanliness depend upon an abundant supply of water (about
30-40 litres per person daily) located near the house and available 24 hours a day for 365
days of the year. Improved cleanliness also depends on the correct use of the water once
it is available, and this behavioural factor is discussed below and on="#page3">page
three. Excreta disposal
|
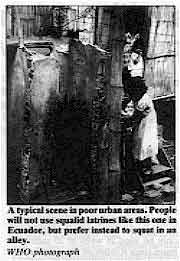
A typical scene in poor urban areas. People will not use
squalid latrines like this one in Ecuador, but prefer instead to squat in an alley.
WHO photograph The main diarrhoea-causing pathogens are shed in the faeces and therefore the hygienic
disposal of human faeces is of the utmost importance. Each family must have access to a
latrine which all members use and keep clean. The latrine must be acceptable and
attractive to the users. Some studies have shown that the construction of latrines does
not necessarily reduce the incidence of diarrhoeal diseases. This is probably because the
latrines were not used, not kept clean, or not used by the most important section of the
community - the children.
|
 |
Behaviour
The provision of good water supplies and latrines will achieve little unless people
understand these new facilities, like them, maintain them and use them. Therefore
all water and excreta disposal projects must be accompanied by vigorous programmes of
community education and must be planned and implemented in cooperation with the community
(see="#page3">page three). The promotion of frequent hand washing may be
especially effective (see="dd02.htm#page3">Diarrhoea Dialogue 2 page three). Focus on children
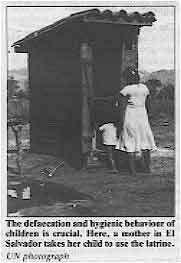 |
The defaecation and hygienic behaviour of children is crucial. Here, a
mother in El Salvador takes her child to use the latrine.
UN photograph Children are not only the main sufferers from diarrhoea, they are also the main source
of infection. Symptomatic and asymptomatic infection rates are highest in children and it
is their faeces which are most likely to spread infection to the rest of the family and
neighbouring households. The defaecation and hygienic behaviour of children is the vital
but neglected component of diarrhoeal disease control programmes. For children under about four years the educational programmes must be directed at the
parents, especially the mothers. For older children, education of both children and
parents is important.
|
The design of educational programmes to change child hygiene will vary enormously from
community to community. However, in many cultures (including my own in England) parents
often believe that the faeces of small children are fairly harmless. It would be
relatively simple to design a programme to convey the message the stools of small
children are dangerous. An integrated approach There is abundant evidence that improving only water quality or only
latrines will have little or no effect on the incidence of diarrhoeal disease. We must
hope, and evidence exists to support this hope, that a combination of improved water
quality, increased water availability, hygienic and acceptable latrines, and vigorous and
sustained educational programmes will be effective. The impact of such an integrated
approach will clearly be different on different types of diarrhoea. For instance, cholera,
typhoid and shigellosis may be substantially reduced whereas rotavirus diarrhoea is likely
to be unresponsive. Nevertheless the goal must be to design affordable and effective integrated programmes
which will reduce overall diarrhoeal disease morbidity and mortality even before there has
been any dramatic reduction in poverty. The most cost-effective mixes of water, sanitation
and education are yet to be defined and are a major priority of the applied research
component of the WHO Diarrhoeal Diseases Control Programme to be described in the="dd05.htm">next issue of Diarrhoea Dialogue. *Organisms which may produce disease.
(1) Levine R J et al 1976 Failure of sanitary wells to protect against cholera and
other diarrhoeas in Bangladesh. The Lancet, July I0 1976: 86-89
(2) Gordon J E, Behar M and Scrimshaw N S 1964 Acute diarrhoeal disease in less
developed countries. Bulletin of the World Health Organisation, 31: 1-28 (3) Feachem R et al 1978 Water, Health and Development. Tri-Med Books Ltd, London (4) Schliessmann D J et al 1958 Relation of environmental factors to the occurrence
of enteric diseases in areas of Eastern Kentucky. Public Health Monograph No. 54.
Washington: U. S. Government Printing Office
|
|
DDOnline
Diarrhoea Dialogue Online Issue 4 February 1981
5 Page 6 7
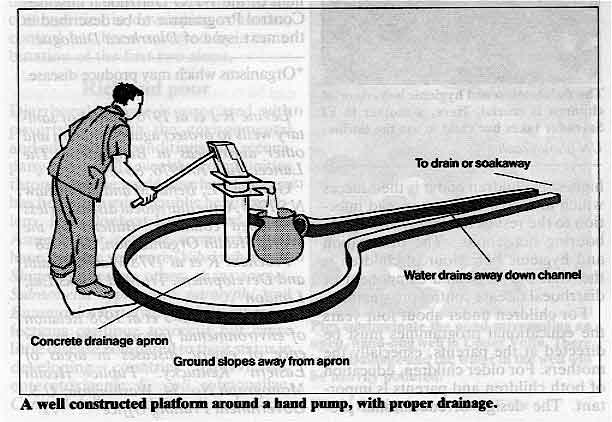
Choosing a hand pump John Cuthbert reports on recent testing of hand pumps The choice of pump must take into account the depth of the well and local conditions,
particularly with regard to maintenance. Many pumps are installed in areas where they
cannot receive the necessary maintenance and therefore stop working after a short time. A
suitable pump should be:
- simple to maintain locally
- easy to repair without using expensive, imported spare parts
- constructed so that it is difficult to steal parts of the machinery.
Other important points:
- there should be as few external fittings as possible, as these can easily be knocked out
of place
- if the water is corrosive, the materials from which the pump is made should be chosen to
minimise the effects
- if the well dries out from time to time, a conventional pump cylinder with leather cups
should be avoided
- otherwise conventional brass cylinders with leather piston cups are quite satisfactory
- the pump must be simple to work. A long handle with a relatively small arc of movement
and a counter-balance weight is easiest to use.
Best buys
The India Mk. II In tests of 12 pumps carried out in the United Kingdom, the India Mk. II pump
was found to be reliable, required little maintenance, was very easy to use and cheap
(£65)*. Its disadvantages are that careful positioning is required in installation and
that it can only be used in wells of 20 metres or more since it relies on the weight of
the water column to carry the piston downwards. The Constallen
 |
The Constallen pump from England is also good value at £170* and uses stainless
steel and plastics in its cylinder for corrosion resistance. It was found to be reliable,
although some wear results from pumping waters containing sand. It is not as easy to use
as the India Mk. II, having a much shorter handle. Installation of the thin and
easily damaged cylinder requires care, and maintenance or repairs to the cylinder could be
difficult in the field.
|
Alternatives
Verguot Hydropumpe 4C2
Other pumps worth considering include the Verguot Hydropumpe 4C2 from France at
about £350 - £400*. This is a foot operated pump which was relatively easy to use,
although women wearing saris or long dresses might have some problems. It seems to be
reasonably reliable and corrosion resistant. However, it is a complex, novel design.
Availability of spares could be a problem and repairs in the field may be difficult. A
well organized system would be necessary for maintenance although this should rarely be
needed. The Mono ES 30
The Mono ES 30, an English rotary pump at £370*, is very strong and reliable
and requires hardly any maintenance. There could be problems in sealing it against
contamination of the well, unless a robust well head is available. It is also easy to push
rubbish into the spout and down the pump. The samples tested gave a poor performance but
the manufacturer claims that the design has now been considerably improved. It is clear that no one pump is suitable for all countries and all situations. Further
evaluation is needed and the World Bank, with United Nations Development Programme
(UNDP)
funds, is now implementing further extensive tests of such pumps around the world. * All prices correct at time of going to press. John Cuthbert is Director of the Water Research Centre, Stevenage,
Herts.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 4 February 1981
6 Page 7 8
Oral rehydration with dirty water?
Many of you have asked about the use of dirty water in making up oral rehydration
solution when clean water is unavailable. Richard Feachem
suggests that the benefits of early replacement of water and electrolytes in acute
diarrhoea far outweigh the possible risk of using contaminated water.
|
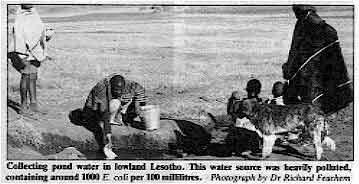
Collecting
pond water in lowland Lesotho. This water source was heavily polluted, containing around
1000 E. coli per 100 millilitres.
Photograph by Dr Richard Feachem Mothers are encouraged to prepare oral rehydration fluid using only clean water.
However, most people in rural areas of developing countries have no access to clean water
and in some communities the only available water is heavily contaminated with faecal
material (1).
|
 |
In these circumstances it is recommended that the water be boiled and allowed to cool
before preparing the oral rehydration fluid. This is often impracticable - involving use
of expensive fuel and delaying the start of treatment. If oral rehydration therapy becomes
common-place in villages it is certain that the oral rehydration fluid will often be made
up with water containing pathogens of faecal origin. Does this matter? The answer is we
don't yet know but it probably doesn't. The main questions
The dirty water used to make up the fluid may contain faecal viruses, bacteria and
intestinal parasites. Of these only the bacteria may multiply if conditions are right.
Oral rehydration fluid is normally used for about 24 hours after it is prepared and
therefore the two central questions are:
- can certain bacterial pathogens that may be present in water multiply in oral
rehydration fluid stored in the home at 20-30°C
- if they can, what is the effect of ingesting a large dose of bacterial pathogens on an
intestine already colonized by the same pathogen or by another viral, bacterial or
protozoal pathogen
Only multiplication (rather than enhanced survival) of a pathogenic bacterium in
oral rehydration fluid is important, since only if multiplication takes place might the
child receive a greater dose of the bacterium in the oral rehydration fluid than in plain
water. Laboratory experiments
The results of laboratory experiments are conflicting. Some have found a steady decline
in the numbers of pathogens introduced into oral rehydration fluid. On the basis of these
findings a WHO Scientific Working Group (2) concluded that "Escherichia coli,
Vibrio cholerae, Salmonella and Shigella do not multiply in oral rehydration
fluid and survive in declining numbers for up to 48 hours". This is unlikely to be true in all circumstances and one recent study has shown that V.
cholerae and enteropathogenic and enterotoxigenic strains of E. coli increased
in concentration by between 1 and 5 log10 units after 24 hours in oral rehydration fluid.
However, all these experiments used oral rehydration fluid made up with distilled water,
or with sterilized surface water and therefore failed to duplicate actual field
conditions. Gambian study A more relevant study on the behaviour of wild E. coli in oral rehydration fluid
made up with well water has recently been reported from The Gambia (3). The concentration of E. coli in well water alone fell slightly during 24 hours
storage (23-30ºC). However, in well water plus oral rehydration salts the concentration
increased by over 2 log10 units. The same study compared the response of children (three
months to four years) receiving oral rehydration fluid made up with well water with those
whose fluid was made up with sterile water. There was no difference in the incidence and
duration of acute diarrhoeal attacks, or in the growth rates, between the two groups. It
was estimated that the E. coli ingested in stored oral rehydration fluid were at
most 5 per cent of the E. coli regularly ingested in food eaten by these children
in The Gambia. A sound strategy
In conclusion, some bacteria may multiply in stored oral rehydration fluid. There is no
evidence, however, that using contaminated fluid increases the incidence, severity or
duration of diarrhoea, and there is one study indicating that it does not. A sound strategy, pending more field research, is to advise mothers to use the cleanest
water available, to boil it where possible and not to keep the oral rehydration fluid more
than 24 hours. To those who express concern at this approach it must be stressed that the
proven benefits of water and electrolyte replacement early in acute diarrhoea far outweigh
the possible risk of using contaminated water. (1) The Lancet, August 2 1980 pp 255-256
(2) Report WHO/DDC/79.3
(3) Transactions of the Royal Society of Tropical Medicine and Hygiene, 1980, Vol. 74, pp
657-662.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 4 February 1981
7 Page 8
Nothing new
I feel there is too little new in Diarrhoea Dialogue. In sending it to us, you
are preaching to the converted and a great many agencies are now disseminating these
ideas. Many people are doubtless not yet enlightened but are they receiving Diarrhoea
Dialogue? For us, only ideas and information that take us further are needed. P. H. Snell, Hopital Protestant, B. P. 115, Dabou, Ivory Coast.
Visual impact You suggest, (Diarrhoea Dialogue 2, page 8), that
after reading the issues be punched and filed -"in this way. the information ... will
always be easily accessible". Accessible to whom, I ask myself. Sadly, relegation to the office desk drawer or the filing cabinet is the common fate of
most potentially useful material. Why not publish a newsheet that can be used as a
wall-chart for all staff and visitors to look at and discuss? If the information produced
is really to be a catalyst for dialogue, as your title suggests, then it should make a
visual impact as well. In this way, the visitor who enters the office to discuss training
of village healthworkers may well exit knowing more about problems of diarrhoea too. Relatively little information is published in Portuguese for those of us working in
Brazil, Angola, Moçambique and Guinea Bissau. Whilst appreciative of the additional cost
of printing in a fourth language, I do think there is a good case for publishing Diarrhoea
Dialogue in Portuguese. Do other Portuguese speaking readers agree with me? P. L. Delahaye, UNICEF, Luanda, Angola.
Weak tea I have found advising mothers to give dehydrated children weak tea the most practical
solution. Making tea involves boiling the water and mothers will always do this. At
the same time they believe there is some medicinal value in the tea so they get more
motivated than giving other plain drinks. P.S. I do not believe one should resort to contaminated water! J. Kagimba, African Medical & Research Foundation (AMREF), P.O. Box 30125,
Nairobi, Kenya.
Dominica Thank you for sending us Diarrhoea Dialogue. We would like to continue
receiving it. In Dominica, oral rehydration therapy was started in the referral hospital in September
1978, and introduced to all health workers in 1979. UNICEF oral rehydration salts packages
became available after hurricane David struck the island on 29th August 1979. The doctors, district nurses and community health workers were informed by lectures, a
seminar and a manual on management of diarrhoea. The public was informed by radio and
newspaper releases, and by a booklet on nutrition in the first year of life, containing
one page about oral rehydration. An explosive outbreak of diarrhoea from February to April 1980 showed clearly the value
of oral rehydration therapy. Of the approximately 2000 children under two years who
suffered from diarrhoea in that period only 99 were admitted to the hospital, of whom only
41 had to be treated intravenously. Both health personnel and the public are very enthusiastic about oral rehydration
therapy, and it has now almost completely replaced the drugs and "bush
medicines" which were used before. J. M. Wit, Princess Margaret Hospital, Goodwill, Commonwealth of Dominica, West
Indies.
Hand washing I have a comment to make on one of the pictures in Diarrhoea
Dialogue 2. On page 3 a child is shown washing her hands. It suggests that all the
children will use the same water (this is often done). It would be better to show the hand
washing with one using a jug or kettle to pour water on the hands of the one washing,
using the bowl to collect water for later disposal. Water can be used quite economically
this way, once the pourers learn to control the flow, a kettle being the slowest pourer. N. M. O'Brien, United Nations Relief and Works Agency for Palestine Refugees, Amman,
Jordan.
Aids for disabled children
One of the most important ideas being spread by the International Year of Disabled
People (IYDP) is that disabled children can do many things for themselves and become
significant members of the community. All children learn through play. Don
Caston* has
designed some simple climbing frames, supports and other aids for disabled children which
make it possible for them to play with others in the village. The aids are very easy to
make and have been in use in developing countries for five years.
AHRTAG has reproduced the aid: as a set of "pop-up" colour pictures on
strong, plasticized paper. This three-dimensional presentation shows very clearly the
purpose of each aid and how it should look when finished. There is no text on the eight
pop-ups but a simple instruction sheet explains how they are made and how they will
benefit disabled children.
The sets are available now.
Please send your money with your order, unless you require more than ten sets, in
which case write to AHRTAG for a quotation on postage and packing.
UK, Europe and the USA: £1.75 (US$ 6.00) for each set including postage and
packing.
All other countries: £1.00 (US$ 3.00) for each set including postage and
packing.
*Handicapped Education & Research Unit, City of London Polytechnic, U.K.
|
|

Scientific editors Dr Katherine Elliott and Dr William Cutting
Executive editor Denise Ayres Editorial advisory group
Professor David Candy (UK)
Dr I Dogramaci (Turkey)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhorn (USA)
Dr D Mahalanabis (India)
Professor Leonardo Mata (Costa Rica)
Dr Mujibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Dr Paul Vesin (France)
Dr M K Were (Kenya) With support from WHO and UNDP
|
Issue no. 4
February 1981
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 August, 2019
|






