|
| |
Issue no. 5 - May 1981
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
Pages 1-8 Diarrhoea Dialogue Online
Issue 5 - May 1981
|
DDOnline
Diarrhoea Dialogue Online Issue 5 May 1981
 Page 1 2
Page 1 2
THEORY INTO PRACTICE
WHO and World Bank activities during the International Drinking Water Supply and
Sanitation Decade. "Water supply and sanitation development must be complementary and developed
with all other aspects of primary health care programmes. This is the approach to the
Decade which WHO has adopted."
For these programmes to be put into practice, major changes in national policy and
management are necessary, which at times may be difficult to achieve. One example of this
is the need to strengthen community-based manpower if projects are to be self-reliant and
self-sustaining. While this approach may be easy to implement in some cases, in others it will not only
require hard work but also the will to accept change. The importance of community
involvement cannot be over emphasized. Technical cooperation
WHO's technical cooperation with member states focuses on:
- the promotion and support of the development of national programmes.
- the identification and preparation of projects for subsequent funding by the World Bank
and other finance institutions.
- the strengthening of national institutions and capabilities.
Specific aspects of cooperation include:
- helping to assess country situations.
- supporting countries in the development of Decade strategies to bring about health
improvements.
- studying problems which may delay progress in the Decade and making recommendations for
improvements.
- identifying, formulating and costing projects.
- strengthening health agency contributions and assimilating primary health care
principles to the provision of water and sanitation.
- organizing "soft-ware" support in manpower, health education for community
involvement, water quality surveillance and control, and the transfer of technology.
Monitoring and evaluating
WHO is helping to:
- monitor the Decade's implementation.
- report on developments for review by the participating agencies.
- coordinate the overall promotion of the Decade through the Steering Committee for
Cooperative Action.
With the help of governments and UNDP resident representatives, WHO also operates a
system to channel information and requests for support from national programmes to donor
countries and vice versa. WHO is also establishing a worldwide programme of information
exchange and is considering the need for evaluation and applied research in support of the
Decade. WHO works mainly through its staff rather than through providing finance for equipment.
Field staff cooperate with national organizations backed up by the six WHO Regional
Offices and the Organization's headquarters. At the present time, there are more than 130
professionals assigned to about 90 countries. Dr B. H. Dieterich, Division of Environmental Health, WHO, Switzerland. "Water supply and sanitation projects must improve:
- the productivity and welt-being of the beneficiaries
- the quality and quantity of water supply and sanitation
- the supply of water and waste disposal for commerce and industry."
The World Bank Group finances projects on a loan and credit basis in developing
countries among its member states. Its lending programme has quadrupled from an average of
less than US$ 200 million between 1970-1975 to an average of US$ 750 million during
1979-1980. Sector investment levels in future years will probably exceed the 1979-1980
figure. Project development
Investment projects must be well prepared, and supported by sound organization and
finance. Project facilities must be appropriate, efficiently built and operated, and well
maintained. In rural areas the community must be able to operate and maintain the new
facility - with the necessary technical assistance from a support organization. Project
beneficiaries should also receive health education and other basic health care - either
from the project organization or other institutions. The World Bank not only finances projects, but also:
- provides funds for the preparation of schemes by governments.
- provides technical expertise (with UNDP financial support) to assist governments in
project design. Such projects usually emphasize the use of appropriate technologies
benefiting the rural and urban poor.
- supports WHO both financially and through assistance with national health sector
programming, health education, basic health care, community action activities and
research, and evaluation of environmental health.
- coordinates with other agencies, such as UNICEF, in the development of projects to
ensure that the organization best qualified in a specific area becomes responsible for the
appropriate projects.
John Kalbermatten, Water and Wastes Advisory Unit, The World Bank, Washington, DC,
USA.
|
In this issue . . .
- WHO and IDRC research programmes in water supply and sanitation
- country profiles from Mozambique and Nepal
- appropriate latrines
|
|
DDOnline
Diarrhoea Dialogue Online Issue 5 May 1981
1 Page 2 3
Disinfecting with sunlight
The potential risks in making up oral rehydration solutions with dirty water were
discussed in Diarrhoea Dialogue 4. One possible way to
overcome this problem is to use the well documented bactericidal properties of sunlight.
In a recent letter to The Lancet (1) researchers at the American University of
Beirut, Lebanon, reported experiments on one litre lots of ORS made up with chlorine free
tap water and sewage. The contaminated ORS was placed in sterile polyethylene bags, some of which were placed
in direct sunlight, some in a room (natural and artificial light) and some in the dark.
The initial concentrations of bacteria were typical of those which might occur if ORS was
made up with water from a heavily contaminated open well or pond (coliforms and faecal
streptococci around 10 / 4 per 100 millilitres). Zero coliform and Strep. faecalis counts
were obtained in one and two hours respectively in samples stored in direct sunlight. The temperature of the ORS did not rise more than 5°C after two hours in the sun and
NaHC03 concentrations and pH did not change. After two hours in the sun the bags were
stored indoors for one day and no regrowth of coliforms was detected. (Coliform reductions
of only 80-85 per cent took place in the bags kept in the dark and in a room for two hours
and, after one day additional storage, massive regrowth had occurred.) These experiments confirm that two hours in bright sunlight in a transparent container
will effectively disinfect small volumes of ORS. (Storage indoors or in a cupboard will
cause an initial decline in faecal bacteria followed by a rise.) The practicality of this
method of disinfecting ORS is doubtful. Do mothers in your community have the appropriate
sealed, transparent containers and do they have somewhere safe to put the bottle in the
sun? What happens on a cloudy day? However, the options for disinfecting ORS in the home are few. Boiling is often not
practicable and chlorine or iodine are typically unavailable. Diarrhoea Dialogue welcomes
correspondence on these, or other methods of disinfecting ORS. (1) Acra A et al 1980 Disinfection of oral rehydration solutions by sunlight. The
Lancet vol. 2: 1257-1258. Teknaf
Very few studies have been undertaken to evaluate the impact of clean, accessible water
supplies and sanitation on the incidence of diarrhoeal diseases in rural communities. Some
of the difficulties associated with this kind of survey are discussed on pages="#page4">four and five of this issue and we hope to consider
the subject further in future issues of Diarrhoea Dialogue.
 |
A hand pump at Teknaf
Photograph by Denise Ayes At Teknaf in southern Bangladesh, a clean water and sanitation intervention has been
underway since June 1980. It is hoped that the programme will have a particular impact on
the health of children under five. Sixty hand pumps have been installed in the
intervention area, with about five or six families using each pump. The pumps are checked
regularly to avoid unnecessary breakdowns. Project staff are studying the way in which
villagers use the pump water.
|
Eight experimental water sealed latrines are already in use in the intervention area
and it is planned to supply one to each family during the next year. A health education
programme promotes proper and continued use of the latrines. Locally made clay
"potties" will be provided for small children who cannot use the adult-sized
latrines. Initial indications from the study of the effect of the intervention on the incidence
of diarrhoeal diseases seem encouraging. A full evaluation will not be available however
until after the study is completed in June 1982. If you would like further information about the Teknaf project, please write to Dr
Mujibur Rahaman, ICDDR, B, PO Box 28, Dacca, Bangladesh. Jamaican study
A recent paper in The Lancet (1) from members of the Department of Child Health,
University of the West Indies, Jamaica raised several interesting points. Their study
compared the composition of salt-sugar solutions prepared by 44 Jamaican mothers according
to "current health education" and those prepared using a double-ended spoon. The authors found that:
- the composition of homemade oral rehydration solutions is often dangerously wrong.
- the osmolality of the glucose/water solution was especially high because mothers
prepared the solution according to taste - and in Jamaica people prefer very sweet and
salty food.
- the two-ended spoon is useful in helping to improve the precision with which oral
rehydration solution is made up. But there are difficulties in measuring unrefined sugar.
A single spoonful yields a concentration of only 1-2 per cent.
Mothers have to be informed about the most accurate way of preparing homemade oral
rehydration solution where WHO packets are hard to obtain, and in Jamaica local radio and
television have proved invaluable in passing on the message. (1) Harland P S E G et al 1981 Composition of oral solutions prepared by Jamaican
mothers for treatment of diarrhoea. The Lancet vol. 1: 600-601. Requests for reprints should be addressed to P S E G Harland at the Dept. of Child
Health, University of the West Indies, Mona, Kingston 7, Jamaica.
|
In the next issue . . .
- the relationship between nutrition and diarrhoeal diseases
- encouraging sick children to eat
- practical advice on breastfeeding
Diarrhoea Dialogue 6 will be available at the end of
August 1981. |
|
DDOnline
Diarrhoea Dialogue Online Issue 5 May 1981
2 Page 3 4
Water supply and sanitation programmes
Sandy Cairncross and Colin Glennie
report from Mozambique and Nepal. Nepal
|
Nepal: using water from invariably faecally polluted
sources
In the hills of Nepal women and girls must walk for several hours up and down steep
paths to collect water from invariably faecally polluted sources. As a result, there are
minimal supplies of poor quality water in the home. Latrines are virtually non-existent;
the village environment is contaminated and, in particular, the home surroundings are
seriously polluted by children's excreta which are highly pathogenic and yet considered
harmless.
|
 |
Gravity water systems
In 1971, the government started a programme of constructing gravity water systems in
small hill communities. The most significant result was that women no longer spent hours
collecting water and the programme stimulated demand all over the country. Despite many
problems, a viable programme now exists where none existed before. Improvement of sanitation
UNICEF in Nepal is focusing its attention on child nutrition. In this context the
reduction of diarrhoeal and worm diseases in children is likely to have a significant
impact on nutritional status. While inadequate water supply remains a serious problem, the
biggest obstacle of all is the lack of sanitation. UNICEF will continue to support the
rural water supply programme, with a major emphasis over the next decade on the
improvement of sanitation in villages. Colin Glennie, UNICEF, Kathmandu, Nepal. Mozambique
Mozambique's greatest advance in the water and sanitation sector has been in the
construction of pit latrines. A country-wide campaign was launched shortly after
Independence by the Ministry of Health and the "dynamising groups" - the local
committees set up by Frelimo as organs of people's power. During two weekends of voluntary work, hundreds of thousands of latrines were built. In
cities such as Maputo, it thus became possible to dispense with the insanitary system
imposed before Independence by which nightsoil buckets were collected by forced
labour. In
the countryside, the campaign has been consolidated by health education (given, for
instance, to patients waiting for treatment at clinics) and by building public latrines
for schools, social centres, etc. In the communal villages, where people who previously lived scattered in the bush are
building a new life together, the vast majority of households already have their own
latrines, which are being used and maintained. Some dynamising groups have even decided to
pass a bye-law that each family must build their latrine before they start to build the
rest of their new home. Concrete slab
Some town dwellers have had difficulty in obtaining suitable materials to cover the
pit. To overcome this problem the Ministries of Health and Public Works have developed a
concrete slab costing less than 500 MT ($ US16). The slightly conical shape makes it possible to eliminate the steel reinforcement on a
slab 1.1 metres in diameter and less than 4 cm thick. The slabs are cast on top of each
other to improve the curing of the concrete and to save space in the neighbourhood casting
yard. Water is most frequently supplied to the communal villages by simple wells with hand
pumps. There is no alternative to this method given the number of people for whom the
government hopes to provide water over the next ten years. Shortage of engineers
Mozambique suffers from a terrible shortage of engineers. Nevertheless, manuals and
special courses have been devised which have permitted technicians with only six months
training to design and build small dams, for instance, and water towers as large as 100
cubic metres. Training is a major feature of the water sector in Mozambique, with a training centre
recently set up in Maputo to produce over 200 junior technicians a year. Another programme
planned for this year will train villagers to carry out simple maintenance tasks on hand
pumps. Sandy Cairncross, Ministry of Works, Maputo, Mozambique.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 5 May 1981
3 Page 4 5
| Environmental health: WHO and IDRC research programmes |
WHO: A major strategy
"A vital long term goal is to develop the most effective methods of
environmental intervention to reduce the transmission of diarrhoeal agents."
(2) The WHO Programme for the Control of Diarrhoeal Diseases was established in 1978 with
the ambitious goal of cooperating with countries all over the world in ". . . a
major attack on the diarrhoeal diseases" (1). The two main
aims are to:
- provide technical and managerial assistance to national health programmes, to enable
them to apply known effective measures for the clinical management and
control of these diseases.
- support research that is likely to lead to new and improved approaches for the
treatment and prevention of diarrhoeal diseases.
Scientific working group
An ad hoc Scientific Working Group (SWG) on Environmental Health and
Diarrhoeal Diseases Control was held in July 1979 (3). This group of experts reviewed in
depth:
- the environmental basis of transmission of enteric pathogens.
- the effect of environmental interventions on diarrhoeal diseases.
- environmental technologies appropriate for the village level.
- behavioural aspects of environmental control of diarrhoeal disease.
- organizational issues in environmental control.
It also discussed priorities for further research in these areas, and noted that
research needs were very varied and differed from much other diarrhoea-related research
because they:
- were multidisciplinary.
- formed a continuum from basic research to applied, operational work.
- were often culture-specific.
Overall priorities
The recommendations of this Group have been taken into account in developing overall
research priorities for the Programme. Two of the three SWGs that have since been set up
to manage basic research - on bacterial enteric infections (4) and viral diarrhoeas (5) -
have included among their priorities a number of research needs relating to environmental
health. These include:
- study of the transmission of bacterial enteric pathogens and of ways of interrupting
their transmission through environmental interventions.
- study of the ability of different water and excreta treatment and re-use processes
(especially those appropriate in developing countries) to remove enteric pathogens.
- development of methods of detecting viral agents of diarrhoea in different environments,
and of the factors influencing their survival and transmission.
- evaluation of the efficacy of various disinfectants and other inactivating agents
against viruses, once these methods become available.
- investigation of the overall adequacy of E. Coli as an indicator of the
presence of bacterial and viral enteric pathogens in aquatic environments in tropical
countries, and of the suitability of faecal streptococci as alternative indicator
organisms.
Field research
The Programme is also pursuing field research directed specifically at the village
level through SWGs established at each of the six WHO Regional Offices. Among the many
research needs are studies of:
- the importance attributed by communities to water supply and sanitation and methods of
mobilizing community participation in these projects.
- the relative effectiveness of different health education techniques for changing
behavioural patterns related to water supply and sanitation.
Uttar Pradesh
In an area in Uttar Pradesh, India, where only limited development activity has taken
place, four groups of villages have been selected for an intensive five year study of the
health effects of continuous, abundant and safe water supplies as opposed to traditional
sources of water. In one group, safe water only has been made available; in another, an adequate
sanitation system has also been provided; in a third, no development has taken place but a
health education programme dealing with personal hygiene and nutrition has been
introduced; and in the fourth, no intervention has been or will be made. Diarrhoeal
disease incidence and mortality are amongst the indicators being used to assess the health
effects. But the task is complicated by the inevitable use of water sources other than
those provided by the project. Sudan
At the "Blue Nile" research and control project in Sudan, a vast and
concerted attack is being made on health problems - mainly schistosomiasis, malaria and
diarrhoeal diseases - linked to irrigation. At the same time as treatment and control
measures are being strengthened in the project area, an effort is being made in one study
zone to:
- determine disease transmission patterns.
- evaluate the cost and effectiveness of control strategies.
- assess the impact on agricultural productivity.
From 1984, new and proven strategies will gradually be introduced to cover the whole
project area. The WHO Programme for the control of Diarrhoeal Diseases is seeking to
encourage work in this field and invites proposals for research. If you are interested,
contact the Programme Manager, CDD Programme, World Health Organization, 1211 Geneva,
Switzerland. Michael Merson, Programme Manager, CDD Programme, World Health Organization, Geneva,
Switzerland.
(1) Diarrhoea Dialogue 1980 No 1: 6
(2) Unpublished document WHO/CDD/ 80.2: 22.
(3) Unpublished document WHO/CDD/ 80.5
(4) Unpublished document WHO/CDD/ BEI/80.2
(5) Unpublished document WHO/CDD/ VID/80.2
|
|
DDOnline
Diarrhoea Dialogue Online Issue 5 May 1981
4 Page 5 6
| Environmental health: WHO and IDRC research programmes |
IDRC: Technology is not the bottleneck
"It is time that new faces and fresh ideas were introduced into the area of
water supply and sanitation if any worthwhile changes are to occur in the coming
decade." The decade 1981-90 has been declared by the United Nations as a period for intensive
action in the field of water supply and sanitation. Apart from the unrealistic targets set
by the 1977 Mar del Plata conference on water, there are several constraints which could
severely jeopardize the major investments to be made in this sector during the coming
decade. These include:
- the dominance of technological approaches planned by engineers who are more interested
in design than in acceptance and proper usage of the technology.
- the lack of hygiene, health and educational programmes to prepare communities for
acceptance of the facilities and ensure proper use after installation. As it is difficult
to alter social behaviour over the short-term, educational efforts are necessary over many
years.
- the little emphasis placed on making communities aware of the importance of improved
water supply and sanitation to the overall quality of life, or of the link between
contaminated water and poor disposal of human excreta on the one hand and diarrhoeal
diseases and skin infections on the other.
- the 'top-down' approach taken by technically oriented water supply and sanitation
agencies in developing countries and the lack of communication between themselves and the
minimal contact with health, social and educational sectors.
- the shortage of manpower at all levels, from professional to village-level technicians.
These problems are aggravated by the outdated curricula and methods used in training
institutions, the lack of community participation and the inability to recover costs and
provide facilities through tariff schemes, resulting in an eventual failure to maintain
the facilities once installed. Shortage of manpower
The Health Sciences Division of the International Development Research Centre
(IDRC),
which has been heavily involved in supporting research activities in the water supply and
sanitation field over the past six years, has recently reoriented its programme. It has
become clear that technology alone is not the bottleneck. Cost, manpower, acceptance and
maintenance at field levels are the crucial factors in the success of a chosen method or
system. In developing countries there is a severe shortage of the manpower needed to carry out
research in this field, thus severely limiting the scope of activities. Therefore,
projects supported in future are likely to have a greater service component than before.
They will also involve personnel from different disciplines. Current projects
The areas presently being developed with investigators and instructors in developing
countries are: The implementation and evaluation of water supply and sanitation technologies
in rural and urban slum areas. The activities undertaken include sanitary
and health components, maintenance and spare parts, acceptance and cost-effectiveness of
the technologies. Social and managerial aspects of water supply. Activities are under way to study
effective tariff schemes and water-use practices. A lack of basic know-how continues to
plague the planning, implementation and execution of water schemes. Manpower development in 1980. Regional seminars were held in Malawi and Botswana
on water supply and sanitation to review improved methods of water delivery and sanitation
disposal with key personnel from planning and training institutes in Ethiopia, Kenya,
Tanzania, Malawi, Lesotho, Mozambique and Botswana. At these meetings, discussion took
place on the broader aspects of education, acceptance and maintenance of water supply and
sanitation programmes and the necessity of updating curricula in training institutions to
broaden the approach in preparing new cadres. Support for seminars to implement changes at country level has also been encouraged.
The possibility is being studied of putting experts in training institutions to work with
trainers in amending the curricula of their programmes. Groundwater extraction and surface water treatment and delivery. Studies are
under way in Panama, Ecuador and Thailand using simple and appropriate technologies to
provide water of reasonable quality and quantity to small, rural communities. Emphasis is
placed on maintenance and community participation. Socio-cultural factors. Projects are being developed in the Philippines and
India to develop guidelines that can be used to obtain information on community attitudes
towards new innovations in water delivery and disposal of excreta. Continued investment
The Division's activities also include studies on varying aspects of diarrhoeal
diseases and the testing of different delivery systems to supply oral rehydration salts to
combat the effects of the diseases in the 0-5 age group. The importance
of improved water supply and sanitation in reducing morbidity and mortality among young
children cannot be overemphasized. It is time that new faces and fresh ideas were introduced into the area of water supply
and sanitation if any worthwhile changes are to be recorded in the coming decade. It must
also be realized in developing countries and among donor agencies that the investment will
be required over two or three generations if there are to be changes in acceptance and use
of facilities. Health Sciences Division, International Development Research Centre, P. O. Box 8500,
Ottawa, Canada K1G 3H9
|
|
DDOnline
Diarrhoea Dialogue Online Issue 5 May 1981
5 Page 6 7
Appropriate latrines
Geoffrey Read describes two types of excreta disposal
systems which are both affordable and appropriate for most developing countries. There are some 2,000 million people in the world today who have no excreta disposal
facilities. These will all have low incomes and are unable to afford piped sewerage.
It may also be technically inappropriate for them. Alternative,
well-proven technologies can be used and, if properly designed, they will safely dispose
of excreta on site, while being both socially acceptable and affordable to the
house-holder. The on-site excreta disposal technologies appropriate for most developing
countries are the Ventilated Improved Pit Latrine (VIP) and the Pour
Flush Waterseal Latrine (P/F). The Ventilated Improved Pit Latrine (VIP)
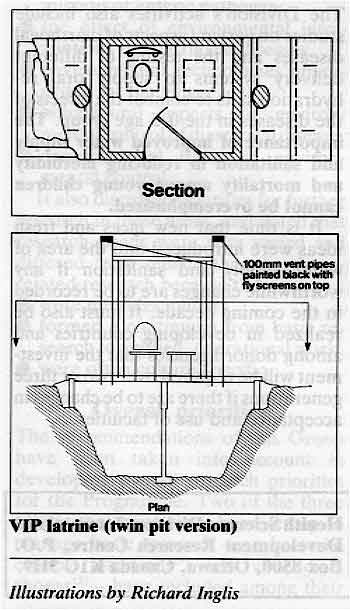 |
VIP latrine (twin pit version)
Illustrations by Richard Inglis
This latrine comprises a seat or squatting plate (depending on cultural preference)
which forms part of a concrete slab over a large pit. The pit is ventilated by a pipe
which is covered at the exit by a non-corrodable insect-proof screen. The pipe removes
odours and gases and is effective in controlling insects which breed in the pit. Removable
concrete covers enable the pit to be emptied when full (pits fill at the rate of between
40 and 60 litres per person per year). The preferred VIP design has twin pits which are used alternately. When one pit
is full, it is rested, and the excreted pathogens die away over time leaving a rich humus.
During this time, the adjacent second pit is used till full. Two years should be allowed
to ensure that the contents of the first pit are pathogen-free. The first pit is then
emptied and re-used and the second pit is rested. In this way the latrine remains in one
position. The householder can construct a building over the pit in any available - but preferably
permanent - material. The pit cover slabs should not be constructed using wood, bamboo or
other materials which will rot. In cases where the water table is high or the ground
unstable it will be necessary to line the pit with brickwork or blockwork, ensuring that
the lined pit remains porous.
|
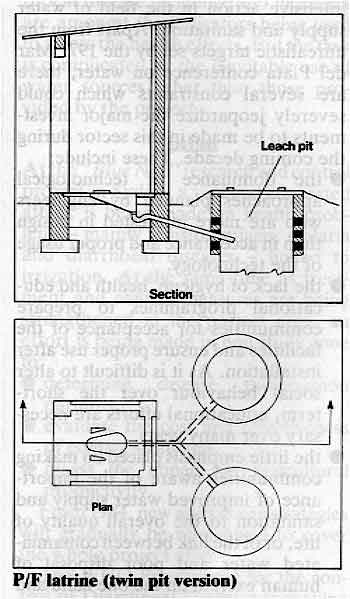
The Pour Flush Waterseal Latrine (P/F)
|
This model comprises a squatting plate and pan over a water seal, connected by
small diameter pipework to an underground leach (filter) pit. The preferred design has
twin leach pits, which are used alternately as with the VIP latrine. Deposited
excreta and urine is flushed away by manually pouring between two and three litres of
water into the pan. The waterseal is thereby maintained keeping out odours, gases and
insects. The leach pits are generally lined with honeycomb brickwork through which liquids
filter away into the ground. The pits fill at about 30 litres per person per year, and are
emptied alternately. In heavy clay soil or impermeable rock, the effluent will need to be
piped away. The P/F is most appropriate in Hindu and Islamic societies where water is used
for anal cleansing. The VIP will give excellent service in situations where water
is in very short supply. When planning sanitation programmes, existing socio-cultural
practices must be carefully considered and the programme tailored accordingly. Provision
should also be made for disposing of dirty wash water, either into a separate soakaway or
into a piped or covered stormwater drain. Latrines should be located as far away as possible from water supplies; if in doubt get
professional advice. Health education, technical support and information programmes are
essential components of sanitation development work. In particular, use by all the family
must be ensured if the sanitation programme is to be successful.
|
 |
The provision and effective use of affordable and appropriate excreta disposal systems
will bring significant long-term health benefits to the millions of people presently
living in unhygienic conditions and continually suffering from gastro-intestinal
infections, high infant mortality and low life expectancy.
Geoffrey Read, World Bank/UNDP Technology Advisory Group (TAG).
|
|
DDOnline
Diarrhoea Dialogue Online Issue 5 May 1981
6 Page 7 8
What are the most useful and easily available sources of
potassium?
N. W. Pirie extends the discussion begun on this page in="dd03.htm#page7">Diarrhoea
Dialogue 3. Bananas are undoubtedly a useful source of potassium (K+). However, it would be a pity
if the tone of the article "Potassium losses and replacement in diarrhoea" (Diarrhoea
Dialogue 3) gave the impression that there are not other good sources where
bananas are scarce or expensive. According to that article, 30g of bananas supply 115 mg
of K+: this agrees with analyses given in food tables. That amount of K+ would be supplied
by 6g of defatted soy flour, 20g of lentils, peanuts or potatoes, and 30g of whole wheat
flour or dark green leafy vegetables (DGLV). Most of the K+ is soluble in water.
|
Bananas are one useful source of potassium, but there are many
others.
Consequently, soy flour should be toasted rather than turned into one of the commercial
"soy felts", and DGLV should be steamed. For the same reason, if 30g of leaf is
thought to be too much for a child, the water in which leaves have been boiled could be
used. That procedure should be avoided if possible because 30g of DGLV would also supply
the daily requirement of carotene (provitamin A) and it, unlike K+, does not come out into
the cooking water.
|
 |
In regions where diarrhoea is common, agricultural residues, dung or wood are the usual
fuels. Few samples of wood ash contain less than 3 per cent K+. It is soluble in water, as
is shown by the old method of making lye (for soap) by dribbling water through wood ash.
The necessary amount of K+ would therefore be present in the extract from 4 or 5g of ash.
The ash from some fresh-water weeds, e. g. water hyacinth, is an even richer source. That
contains 20 to 30 per cent K+ (1,2) and has sometimes been used in place of salt. (3) The
ashes from several by-products of food plants contain similar amounts (4). The conclusion
is that, wherever land plants grow, there must of necessity be a supply of K+. (1) Finlow R S 1917 Water hyacinth and its value as fertilizer. Government Printer,
Calcutta, India
(2) Chokder A H 1968 Further investigations on control of aquatic vegetation in fisheries.
Agric. Pak. 19: 101
(3) Schultz H 1962 Brazil's big-lipped Indians. National Geographic Magazine 121 (1): 118.
(4) Kuhnlein H V 1980 The trace element content of indigenous salts compared with
commercially refined substitutes. Ecology of Food and Nutrition vol 10:113-121. Aspirin and diarrhoea
The use of anti-secretory drugs such as aspirin in diarrhoeal disease control
programmes has been discussed in medical journals recently and several readers have
requested a short comment on this. The role of therapeutics will be more fully examined in
Diarrhoea Dialogue 8.
 |
Children with diarrhoea need rehydration, prevention of further
dehydration and nutrition.
Diarrhoea usually results from excessive small bowel secretion or a failure of
intestinal absorption. Various drugs reduce the rate of secretion, or enhance absorption,
and aspirin is one of them. In a study carried out in Indonesia, 82 children with moderate
or severe dehydration due to diarrhoea were given the same rehydration and supportive
treatment. They were divided into three groups, one receiving soluble aspirin in a dose of
25mg/kg/day in divided doses, another a placebo and the third no additional treatment. The
aspirin group showed significant decrease in stool volume and weight gain compared with
the placebo group (1).
|
Reduction of faecal loss with such a well known drug as aspirin has immediate appeal.
However, the authors of the Indonesian study indicate that the mechanism of aspirin's
anti-secretory activity is unknown. They emphasise the need for further assessment of
possible side effects even though they did not find gastrointestinal bleeding or metabolic
acidosis in the 31 children who had aspirin. In addition, the study was performed under
close hospital supervision which is unavailable to most children in areas where diarrhoea
is common. The dangers of overdosage and toxic effects of aspirin are real and using a
"medicine" may detract from the more important and well-tested technique of oral
rehydration to replace fluid losses. (1) Burke V et al 1980 Reduction by aspirin of intestinal fluid loss in acute
childhood gastroenteritis. Lancet 1: 1329-1330. Norbert Hirschhorn comments on another drug which has been shown to reduce
intestinal secretion:
The use of anti-secretory drugs in a comprehensive diarrhoeal disease control programme
has possibilities. For example, one study showed that chlorpromazine, in non-sedative
doses, reduced stool output in a handful of adults with cholera (2). However, these
results cannot yet be generalized beyond the confines of the immediate study, and it would
be dangerous to assume that drugs alone are sufficient treatment for diarrhoea. Children
with diarrhoea need rehydration, prevention of further dehydration and nutrition. (2) Babbani G H et al 1979 Chlorpromazine reduces fluid loss in cholera. The
Lancet vol 1: 410-412.
|
|
DDOnline
Diarrhoea Dialogue Online Issue 5 May 1981
7 Page 8
Finger-pinch method
I have been working in Nepal in general medicine and
paediatrics. We have experimented
with using a hospital ward as a rehydration unit, with a major emphasis on getting the
relatives to make an oral rehydration solution themselves (rather than the nurses doing it
all for them). We have used the finger-pinch method with good clinical results (though our
measurements of the actual mass of NaCl and NaC03 showed that nearly always a much smaller
amount was being used than WHO recommends). From the little clinical biochemical information we had available we have been teaching
that honey (fructose) is as effective as sucrose. During our diarrhoea season, which is
the dry season from April-May, there is very little fruit available, and it is difficult
to recommend a readily available source of potassium for use in the villages.
J. H. Sleggs, Thimpu General Hospital, Bhutan.
Editors' note:
N. W. Pirie has suggested some useful and easily available sources of potassium on="#page7">page seven of this issue.
Technological approach
I enjoyed reading="dd03.htm">issue three of Diarrhoea Dialogue and
found much useful information in it. We are a comprehensive health service serving a large region of scattered, remote small
Indian villages in northern Ontario. Due to poor socio-economic conditions, diarrhoeal
diseases are common causes of morbidity though, fortunately, not of mortality. Being in a
developed country, medical workers here tend to approach the diarrhoeal diseases in a
technological manner - i.e. heavy reliance on intravenous hydration and mathematical
precision in electrolyte balance. T. K. Young, Medical Director, Sioux Lookout Zone Hospital, P. O. Box 1500, Sioux
Lookout, Ontario, Canada P0V 2T0. Traditional water purification
I found the advice of Dr Kagimba (letters, issue four) not
to resort to contaminated water and to use "weak tea" as a practical alternative
very important. In southern India (Kerala and Tamil Nadu) people prepare boiled waters
known there as "chukku vellam", "jeera vellam" or "malli
water" which are spiced with the seeds of cumin (Cuminum cyanumum), coriander
(Coriandrum sativum) and sometimes also with dried ginger and some sugar. Some mothers
insist that even healthy children should not drink "untreated water" before the
age of ten. Spiced water is not "tasteless" like ordinary boiled water, cumin
seeds are used for the treatment of chronic diarrhoea, coriander seeds are useful for
dyspepsia and Zingiber sp. acts as a stimulant in cases of diarrhoea.
|
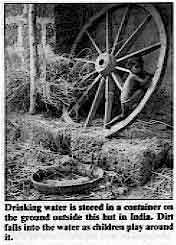
Drinking water is stored in a container on the ground outside
this hut in India. Dirt falls into the water as children play around it.
If the water available is polluted surface water from rivers, ponds or shallow wells it
should be treated first by traditional water coagulation. Details about such simple
indigenous household methods and their scientific assessment are given in a manual
entitled "Traditional Water Purification in Tropical Developing Countries" which
I recently compiled. It will be published by GATE (German Appropriate Technology Exchange,
Eschborn, West Germany). I am very interested in learning more about these practices, because what I have
collected to date is far from complete. In case any readers of Diarrhoea Dialogue know
something about local attempts at water improvement I would be grateful if they could
write to me.
|
 |
During a forthcoming pilot project on the implementation of improved water treatment
methods at household level in Sudanese "model villages" I will ask my
collaborators to incorporate teaching about treatment of children with diarrhoea in their
"health education" on water treatment and hygiene. Especially during the rainy
season when the incidence of gastro-intestinal disease is much higher than at other times
this will hopefully be a valuable supplement. Samia Al Azharia Jab, Water Purification Project, P. O. Box 2681, Khartoum, Sudan.
Critical information
What I like about your newsletter is that it highlights data that are all too often
left out of "scientific" papers. For example, the idea that children are not
only the group most susceptible to and endangered by diarrhoeal infections but that they
are also the most likely to spread the infection because of the less stringent taboos on
where they defaecate (Diarrhoea Dialogue 4, page five). A further example from issue four: the need for more "steal-proof' parts of hand
pumps (page six). And finally, you are willing to face the
"real world". Is it better to rehydrate with less than "pure" water or
not rehydrate at all? Keep on with this kind of critically meaningful information. Dana Raphael, The Human Lactation Center Ltd, Westport, Conn., U.S.A. We are a comprehensive health service serving a large region of scattered, remote small
Indian villages in northern Ontario. Due to poor socio-economic conditions, diarrhoeal
diseases are common causes of morbidity though, fortunately, not of mortality. Being in a
developed country, medical workers here tend to approach the diarrhoeal diseases in a
technological manner - i.e. heavy reliance on intravenous hydration and mathematical
precision in electrolyte balance.
T. K. Young, Medical Director, Sioux Lookout Zone Hospital, P. O. Box 1500, Sioux
Lookout, Ontario, Canada P0V 2T0.
Traditional water purification
I found the advice of Dr Kagimba (letters, issue four) not
to resort to contaminated water and to use "weak tea" as a practical alternative
very important. In southern India (Kerala and Tamil Nadu) people prepare boiled waters
known there as "chukku vellam", "jeera vellam" or "malli
water" which are spiced with the seeds of cumin (Cuminum cyanumum), coriander
(Coriandrum sativum) and sometimes also with dried ginger and some sugar. Some mothers
insist that even healthy children should not drink "untreated water" before the
age of ten. Spiced water is not "tasteless" like ordinary boiled water, cumin
seeds are used for the treatment of chronic diarrhoea, coriander seeds are useful for
dyspepsia and Zingiber sp. acts as a stimulant in cases of diarrhoea.
|
Drinking water is stored in a container on the ground outside
this hut in India. Dirt falls into the water as children play around it.
If the water available is polluted surface water from rivers, ponds or shallow wells it
should be treated first by traditional water coagulation. Details about such simple
indigenous household methods and their scientific assessment are given in a manual
entitled "Traditional Water Purification in Tropical Developing Countries" which
I recently compiled. It will be published by GATE (German Appropriate Technology Exchange,
Eschborn, West Germany). I am very interested in learning more about these practices, because what I have
collected to date is far from complete. In case any readers of Diarrhoea Dialogue know
something about local attempts at water improvement I would be grateful if they could
write to me.
|
|
During a forthcoming pilot project on the implementation of improved water treatment
methods at household level in Sudanese "model villages" I will ask my
collaborators to incorporate teaching about treatment of children with diarrhoea in their
"health education" on water treatment and hygiene. Especially during the rainy
season when the incidence of gastro-intestinal disease is much higher than at other times
this will hopefully be a valuable supplement. Samia Al Azharia Jab, Water Purification Project, P. O. Box 2681, Khartoum, Sudan.
Critical information
What I like about your newsletter is that it highlights data that are all too often
left out of "scientific" papers. For example, the idea that children are not
only the group most susceptible to and endangered by diarrhoeal infections but that they
are also the most likely to spread the infection because of the less stringent taboos on
where they defaecate (Diarrhoea Dialogue 4, page five). A further example from issue four: the need for more "steal-proof' parts of hand
pumps (page six). And finally, you are willing to face the
"real world". Is it better to rehydrate with less than "pure" water or
not rehydrate at all? Keep on with this kind of critically meaningful information. Dana Raphael, The Human Lactation Center Ltd, Westport, Conn., U.S.A.
|

Scientific editors Dr Katherine Elliott and Dr William Cutting
Executive editor Denise Ayres Editorial advisory group
Professor David Candy (UK)
Dr I Dogramaci (Turkey)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhorn (USA)
Dr D Mahalanabis (India)
Professor Leonardo Mata (Costa Rica)
Dr Mujibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Dr Paul Vesin (France)
Dr M K Were (Kenya) With support from WHO and UNDP
|
Issue no. 5
May 1981
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 August, 2019
|






