|
| |
Issue no. 24 - March 1986
pdf
 version of this Issue version of this Issue
|
There is much information in this issue that is valuable
and useful. Online readers are reminded, however, that treatment guidelines and health
care practices change over time. If you are in doubt, please refer to
WHO's up-to-date Dehydration Treatment
Plans.
|
updated: 23 April, 2014
Pages 1-8 Dialogue on Diarrhoea Online Issue 24 -
March 1986
|
DDOnline Dialogue
on Diarrhoea Online Issue 24 March 1986  Page 1 2
Page 1 2
Maintaining the momentum
At the Second International Conference on Oral Rehydration Therapy (ICORT II), held in
Washington D.C. in December 1985, 1,200 participants from some 100 countries exchanged
experiences of implementing ORT. The Conference was officially opened by Mr Peter
McPherson, Administrator of the Agency for International Development (USAID), who recalled
the goals set out at ICORT I, held in June 1983, and described the significant progress
made since then:
- ORT is now widely recognised as appropriate and desirable at all levels of the health
system.
- Many countries have developed policies and plans to address the diarrhoea problem.
- Mothers are now regarded as the key to the treatment of diarrhoea.
- There is agreement that integrated communication channels, such as face-to-face, print,
and radio and television, are necessary to promote ORT messages.
He also stated that ICORT II had been organised through the recognition by USAID and
other international agencies that there was a need for an international forum "for
ORT implementers to share their experiences and discuss ways to overcome the major
barriers to implementing programs in the field". During the Conference, sixty-five countries displayed country posters showing both the
challenges they face and their achievements. Six workshops discussed communications and
social marketing; distribution and logistics; health manpower training; supervision and
monitoring; evaluation and cost issues; and integration of ORT with other health
activities. The conclusions which emerged from these workshops are referred to on="#page5">page five of this issue. We have focused on the main theme of the
Conference - implementation - in particular on areas in which further improvements in the
delivery and acceptance of ORT are still needed. Highlights from speeches by Dr Halfdan Mahler, the Director General of the World Health
Organization, Mr James Grant, the Executive Director of UNICEF, and from the keynote
address by Dr Mamdouh Gabr, the former Minister of Health for Egypt, in which he described
the main factors behind the success of the Egyptian programme, are featured on="#page3">pages three and four. In addition, we have included
brief accounts of what was said by the main speakers, including the excellent summary of
the Conference by Dr Michael Merson, Director of the WHO Diarrhoeal Disease Control
Programme. Summing up ICORT II In his inspiring closing remarks, Mr McPherson described the major conclusions emerging
from ICORT II, and ways in which the lessons learned since ICORT I can be used to extend
the outreach of ORT: "At ICORT I, I think it is fair to say that we reached a
scientific consensus about ORT. At ICORT II from all I've seen and heard, we have taken a
leap forward and achieved consensus for action. I'd like to highlight just a few of the
important points raised:
- You have said here that ORT has changed the face of health care delivery. You have
applied your best creative energies and developed innovative solutions to some incredibly
difficult problems.
- You have said that ORT has led health care out of the clinics and into communities and
homes. We know now that new communications and marketing techniques can revolutionise the
delivery of health services. We now see the importance of political and community
mobilisations.
- You have shown how the private sector can play a pivotal role.
- You have proven that dramatic results can be achieved.
- We have also learned that ORT by itself is not enough.
Now it is time to look to the future. ORT can lead the overall development of health
care. It shows that worldwide coverage of essential health services is in fact possible.
And by reaching into every home and community - ORT can catalyse the very process of
development." Mr McPherson closed ICORT II by urging participants to forge country plans, share
experiences and take the lead in ensuring that donor activity is coordinated, in order to
be able to meet the following targets:
- accessibility of ORT to every child who needs it by 1990;
- a forty-five per cent usage rate of ORT by 1990; and
- the prevention of two million deaths from dehydrating diarrhoea by 1990.
He concluded by saying "ORT programs could be the engine to drive primary health
care to the far reaches of every country", reaffirmed USAID's commitment to future
support of ORT, and raised the possibility of holding a third ICORT at a future date.
|
In this issue . . .
- Promoting ORT: the community pharmacist and the traditional healer
- DD reports on the Second International Conference on Oral Rehydration Therapy
|
|
DDOnline Dialogue
on Diarrhoea Online Issue 24 March 1986 1 Page 2 3
Water conference 1988
The Vlth International Water Resources Association World Congress will be held in
Ottawa, Canada, from 29 May to 3 June, 1988. The overall theme for the congress is
"Water for World Development". For information on abstracts, submissions and
attendance, please write to The Secretariat, Sixth IWRA World Water Congress on Water
Resources, University of Ottawa, 631 King Edward Avenue, Ottawa, Ontario, K1N 6N5, Canada. ICORT II* Proceedings from the Second lnternational Conference on Oral Rehydration Therapy,
containing full texts of all the presentations, will shortly be published. Details of
availability will be included in DD.
 |
The display exhibited by the Malawi CDD programme. One of the highlights of ICORT II was the country poster sessions, where country
programme managers displayed photographs, charts and data explaining their national
diarrhoeal disease control activities. This photograph shows the display exhibited by the
Malawi CDD programme.
|
|
| Publications Salubritas
Salubritas is a quarterly newsletter which provides practical information on health
care for developing countries. Aimed at health workers who are working with limited
resources, the newsletter has useful information on publications and other resources,
training programmes, conferences, news, "how to" pages and feature articles. It
is published jointly by the American Public Health Association and the World Federation of
Public Health Associations.
Subscriptions are US$ 10.00 per year including postage. Bulk copies of eight or more
are available at US$ 8.00 each. A limited number of copies are available free of charge to
health workers in developing countries who cannot afford to pay. Please contact: Salubritas,
APHA, 1015 15th Street, N. W. Washington D.C. 20005, USA.
WHO/UNICEF statement
The second edition of the joint WHO/UNICEF statement (identified by a yellow stripe on
the cover): The Management of Diarrhoea and Use of Oral Rehydration Therapy has
recently been published. The most obvious change is the substitution of the modified ORS
formula (with trisodium monocitrate replacing bicarbonate). It is available from the Programme
Director, CDD Programme, WHO, 1211 Geneva 27, Switzerland and costs Sw. fr. 3.
Health communication
A special issue of Development Communication Report (DCR) - devoted to health
communication - is available free of charge to readers, from Development Communications
Report, Clearinghouse on Development Communication, 1255 23rd Street, N.W. Washington DC
20037, USA.
Breastfeeding - two new books
Helping Mothers to Breastfeed, by F. Savage King, published by the African Medical
and Research Foundation is now available from AMREF, PO Box 30125, Nairobi, Kenya or
Teaching Aids at Low Cost (TALC), P. O. Box 49, St. Albans, Herts AL1 4AX, U. K. Price:£2.70
plus postage and packing. A slide set, "Breastfeeding Problems", which
illustrates much of the book is also available from TALC. Prices start from £2.00 for
developing countries and £2.50 for developed countries, plus postage and packing.
Breastfeeding matters: What we need to know about infant feeding, by M. Minchin,
published by Alma Publications and George Allen and Unwin, is a practical,
well-illustrated book now available from No. 8 Napier Street. North Sydney, 2060,
Australia. Price: $12.00 Australian, plus postage ant packing (reduced price per copy for
bulk orders).
|
Training for ORS production
The United States Agency for lnternational Development (USAID) is sponsoring a project
to increase the availability of ORS through the private sector. Project SUPPORT is managed
by the Program for Appropriate Technology in Health (PATH), an international US-based
non-profit organisation. One of the project's aims is to increase the pool of technical
expertise in ORS production. Project SUPPORT's programme will include field training and
experience for appropriate candidates. Applicants should have the following
qualifications: a background in pharmaceutical production, chemical, industrial or food
processing; good analytical, writing and interpersonal skills; language facility in French
and/or Spanish. Small business enterprise work and developing country experience will be
given preference. A curriculum vitae and a technical writing sample should be sent to: Director,
Project SUPPORT, PATH, 130 Nickerson Street, Seattle, WA 98109, USA. Erratum The front cover photograph of="dd23.htm">issue 23 of DD should have
credited Dr Jay McAuliffe in addition to Dr Richard Guerrant. The editors would like to
apologise to Dr McAuliffe for omitting his name and belatedly acknowledge his
contribution.
|
|
DDOnline Dialogue
on Diarrhoea Online Issue 24 March 1986 2 Page 3 4
A global strategy WHO
Dr Mahler emphasised the devastating impact that diarrhoeal disease still has on the
health of children in the developing world, and outlined the prime concerns of a global
strategy to implement ORT and its implications for health development.
- ORT and diarrhoeal disease control must be part of a broader strategy for health
development, which requires: "a combination of social action, infrastructural
development starting with primary health care and use of appropriate and affordable technologies"
and integration of the health, education, rural and urban development, and water resources
development sectors.
- " Improvements in health" . . . require . . . " appropriate and
enlightened support from the international community."
- The contribution that successful ORT can make to primary health care "opens the
way for the mother to be convinced of other important measures for disease control and
also gives mothers and other family members confidence in their ability to care for
themselves."
- ORT "links the treatment of disease and the need for good nutrition." Oral
rehydration therapy in the total sense must include "the administration of locally
available, easily digestible foods in quantities greater than normal during and especially
after the diarrhoeal episode."
- The '"successful implementation of diarrhoeal disease control programmes" .
. . requires sound programme planning, careful attention to programme management, due
emphasis on monitoring and supervision and practical evaluation.
- "Proper use of ORT and application of other diarrhoeal control strategies also
require sound operational research ". . . there is also a need to "strengthen
the capabilities of national institutes . . develop more effective oral rehydration
solutions . . . identify those nutrients that are best absorbed during and after
diarrhoea." Operational research into interventions such as "vitamin A
distribution, innovative ways to prevent shigellosis, vaccines for rotavirus, cholera and
typhoid fever" is needed.
Dr. Mahler concluded on an optimistic note: "after only five years, more than
one third of the children in developing countries worldwide already have access to oral
rehydration salts. Use of these salts has saved at least 200,000 lives this year. " UNICEF Mr Grant outlined UNICEF's commitment to child survival programmes, particularly
diarrhoeal disease control, and suggested that we can be optimistic about the prospects
for child survival, provided that the breakthrough of medical knowledge about ORT is
followed by a similar breakthrough in social organisation. He emphasised that:
- While figures show that in many countries child mortality is still unacceptably high,
ORT and immunisation, among other methods, can lead to impressive reductions in the number
of child deaths.
- "The new capacity for social mobilisation to communicate to and involve parents
in these methods" through improvements in and widespread availability of
communications, channelling of knowledge through organisations such as mothers and
agricultural groups, and schools is crucial. "The challenge we face is how to
mobilise the full range of these sectors that influence and affect people's lives. "
- "The front line of health is the family itself. And really what the
technological advances have done is make it clear that these technologies simply give us a
whole new capacity for self-health by and for families if, and only if the societal
structures of the world will help the parent to turn the key." "UNICEF sees the
potential . . . for an unprecedented breakthrough in the health of children over
the next five or ten years. This cannot be achieved without a massive breakthrough on the
diarrhoea front."
|
Implementation questions
DD readers may like to consider the following questions which were put to the ICORT
workshop participants by Anne Tinker, Chief, Health Services Division, USAID, in her
speech Introduction to Implementation Issues. In communications and social marketing
- How can lessons learned from successful mass programmes be transferred to other
countries, most cost-effectively?
- What messages will convince mothers about the importance of feeding, particularly extra
feeding during the convalescent period?
- How to convince mothers that giving purgatives and starving children are harmful
traditional practices, and how to persuade doctors to use ORT and stop using harmful
antidiarrhoeals?
- How to convince mothers not yet using ORT to give a new treatment at home, which does
not stop the diarrhoea, and to continue to use it effectively?
- How to involve channels outside the formal health sector such as school teachers,
churches, students and private industry to more effectively promote ORT?
In logistics and distribution
- How to ensure sufficient supply to meet the demands created by communications
programmes?
- How to best decide on the balance between home solutions and packets to deal with the
estimated one billion episodes of diarrhoea a year?
- How to cope with the cost of packets to health ministries but avoid cutting off the
poor, if packets are sold in the private sector?
- The need to know more about the risks and benefits of flavoured ORS (which comprise
about one third of the commercial market).
In health personnel training
- To what extent mothers, midwives and traditional healers can be trained to be local
dispensers of ORT.
- The best way to involve pharmacists.
- How to ensure that ORT training is linked with subsequent supervision once the trainee
goes home, so that the training is put into action?
In supervision and monitoring
- How best to supervise and monitor the effectiveness of health workers, and how to
supervise and monitor mothers giving home solutions?
In evaluation and cost
- How to meet the needs of those who cannot or will not buy ORS packets but avoid
undermining sales through commercial channels by free distribution of packets.
- Development of new operational research techniques and study techniques to evaluate the
effectiveness of diarrhoeal disease control, in the home and the community.
- How to measure the impact of factors outside the ORT programme on its success.
- What is the least expensive approach that will still produce the required impact?
ORT and other health interventions
- How to ensure that ORT programme activities and benefits are sustained beyond the life
of a donor supported project. If integration is the key to this, how to best integrate ORT
into other primary health care activities.
- How to best provide the range of interventions needed?
|
|
DDOnline Dialogue
on Diarrhoea Online Issue 24 March 1986 3 Page 4 5
| ICORT II: excerpts from the keynote speeches |
|
Effective implementation of ORT programmes Since 1983, the use of ORT has expanded world-wide to more than 95 countries in the
developing world, and there has been a four-fold increase in the number of packets
produced. Of ORT, Dr Gabr said: "Never in the history of medicine has so much been
done for so many with so simple a technology and so little expenditure." With
particular reference to the Egyptian experience, Dr Gabr outlined the essential elements
for effective implementation of a national ORT programme. There must be:
- Co-ordination at country and local levels
- Integration of ORT programmes into the primary health care system
- Tailoring of ORT programmes to national and local socio-economic, cultural and
ethnographic conditions.
- Social marketing
- ORT and the health profession:
- Health personnel should be involved from the beginning in all activities of the ORT
programme.
- The co-operation of doctors is essential for the success of ORT - they are respected and
listened to in most developing countries, even where traditional healers are still
prevalent.
- Medical curricula should be quickly changed to advocate ORT, and to stimulate doctors'
interest by discussion of the scientific background of the absorptive intestinal
mechanisms. Since diarrhoea is so rare in the developed world, western textbooks, commonly
used by medical students in developing countries, often lack information on ORT.
- Research which indicates the uselessness and possible harm of antibiotics for most
pathogens associated with watery diarrhoea is necessary.
- Pharmacists also need to be convinced and given a reasonable incentive to sell ORS
packets as opposed to the profits made from selling other drugs.
- Governments need convincing of the cost-effectiveness of ORT - and the reduction of the
burden on hospital services. Successful programme implementation requires political
commitment.
|
Diarrhoea is a nutritional disease Dr Jon Rohde took the theme "diarrhoea is a nutritional disease" in his
keynote speech and his conclusions are outlined below. "Even successful ORT programmes that have case management strategies limited to
rehydration, to fluid therapy alone, will continue to face large numbers of deaths
associated with diarrhoea . . . unless they deal with the nutritional problems
associated with diarrhoea as well. The failure of nutrition rehabilitation efforts to
"cure" malnutrition . . . suggests that . . . the problem should be dealt
with before malnutrition develops, during the first year or two of life." Dr. Rohde suggests that growth faltering is one of the most useful diagnostic signs of
the onset of malnutrition and that growth monitoring is an appropriate tool for
nutritional assessment. Diarrhoea management must focus, using growth monitoring as a
tool, on the whole child, to counteract the devastating effect of diarrhoea on growth. In
the diarrhoea-malnutrition interaction, the severity and duration of diarrhoea is greater
in the malnourished child, and results in the highest mortality in this group of children.
He also suggests that diarrhoeal deaths could be halved if the increased risk associated
with malnutrition is removed. In fact "in a well running ORT programme, deaths of
these malnourished children are likely to be the only ones which occur. While the problems
of malnutrition seem to be greatest after the age of two years, deviations from the growth
curve occur most frequently between the age of six and eighteen months. The peak incidence
of diarrhoea occurring at the same time as the peak incidence of growth faltering cannot
be dismissed as a coincidence." Feeding and diarrhoea Dr Rohde stressed the importance of feeding both during and after diarrhoea, and the
particular importance of growth monitoring during the catch-up period. Growth monitoring
is important as a visible indicator to convince mothers of the importance of correct and
continued feeding. "Diarrhoea is just not recognised for its contribution to
creeping malnutrition. Once stools become normal, the illness is over. Successful feeding
is demonstrated by the visual record of adequate growth, encouraging the mother to
continue it . . but growth monitoring must be more than just the measurement of
growth. It requires an effective response by the mother." Interventions for diarrhoea control Dr Richard Feachem discussed both the effectiveness and costs of non-clinical
interventions for diarrhoeal disease control programmes (rather than for individual
children). His findings and conclusions are based on extensive literature reviews and
mathematical calculations. The following are those interventions for which evidence of high effectiveness and
feasibility is reasonably strong:
- Promotion of breastfeeding
- Improving weaning practices
- Rotavirus, cholera and measles immunisation
- Improving water supply and sanitation facilities
- Promoting personal and domestic hygiene
Conclusions "Not all interventions are appropriate everywhere. For instance, in rural India it
would not in general be necessary to promote breast feeding, whereas in Latin America and
in urban areas throughout the world, this intervention is likely to be a highly
cost-effective method of controlling diarrhoea morbidity and mortality. In Latin America
cholera vaccination would not be appropriate and indeed, in most countries it will be much
less cost-effective than the data for Bangladesh suggests. Each country must decide for
itself which package of interventions is likely to be most effective and feasible. The
three educationally-based interventions aimed at improving breastfeeding, weaning and
hygiene are not being vigorously carried out in most countries today. There is great scope
for new initiatives in this field, with carefully designed and targeted messages being
delivered through multiple channels. The techniques of social marketing may have much to
offer. Further research into new vaccines and field testing will be necessary before
rotavirus or cholera immunisations are routinely included." For derails write for reprints to Dr Richard Feachem, London School of Hygiene and
Tropical Medicine, Keppel Street, London WC1E 7HT.
|
|
DDOnline Dialogue
on Diarrhoea Online Issue 24 March 1986 4 Page 5 6
| ICORT II: excerpts from the keynote speeches |
ORT: the future Dr Norbert Hirschhorn discussed the causes and processes of diarrhoeal disease, and
the potential of a "super oral rehydration solution". "We now have three ways to proceed in implementing super-ORS, the medicine to slow
down diarrhoea while it rehydrates. One: let us find the optimal combination of chemicals (amino acid, dipeptide,
glucose, or polysaccharide) and with the ORT salts package it as a medicine. Two: "Let us use food! Cereal grains, especially rice, can reduce stool
loss by about 33-50 per cent when 50 grammes are used in a litre of oral rehydration
solution in place of glucose (these data courtesy Drs. Molla of ICDDR, B). Rehydration is
faster, and the solution tastes fine! If we pre-cook ground rice and add suspending
agents, it may be possible to make an ORS that stays in suspension even in cold
water. Preliminary data suggest that maize, millet, sorghum, may be comparably effective. The third way is for mothers to prepare salt-cereal solutions at home. This
approach has the usual advantages and constraints of any home-prepared solution. But be
aware: rice powder is not the same as rice water. Rice water has not nearly enough
carbohydrate or protein." Cereal ORS "Are there problems with cereal-ORS? Some children under three months old don't
digest cereal easily and would get worse diarrhoea; some mothers may take this low-calorie
milky fluid to be food and continue only this; if the solution is prepared with too little
water, the rapid absorption of sodium by super-ORS may make hypernatremia more of a
problem. Overriding these problems, perhaps, is the likelihood that mothers will more
readily accept cereal-ORS and use it well. We need much more experience. I predict
super-ORS will have far greater effect than just slowing down diarrhoea." Chronic/prolonged diarrhoea "Chronic or prolonged diarrhoea has become an increasingly serious problem,
especially as famine and poverty spread. Malnourished children have diarrhoea longer (not
necessarily more often), and prolonged diarrhoea makes children more malnourished. We
worsen the process by fasting the child, using antibiotics (now proved to prolong most
cases of diarrhoea) and by prescribing anti-motility drugs." *Please see="#page2">page page
2 Highlights and conclusions Dr. Michael Merson, Director of the WHO Diarrhoeal
Diseases Control Programme, summarised very succinctly in his address on the last day of
the conference, the highlights of ICORT II, including the major conclusions of the six
workshop panels. At ICORT II we have been shown . . the key characteristics of successful national CDD
programmes. I believe these can be summarised as follows:"
- CDD programmes that have been successful have been founded on a strong political
commitment.
- They have adopted a clear strategy for the delivery and use of ORT in the home and in
health facilities, which includes recommendations for feeding during diarrhoea.
- They have given due consideration to ensuring that adequate supplies of ORS packets are
available when they are needed, through government and commercial channels, and that
pharmacists and traditional practitioners receive training in the proper use of ORT.
- They have given special attention to communications activities orientated towards the
needs of consumers, not just providers of health care.
- They have recognised the importance of supervision, including the regular monitoring of
both the quantity and quality of programme activities.
- They have had a plan for their evaluation from the outset.
These factors were brought out by the workshop participants, who also identified
some of the unexpected constraints that may be encountered in programme implementation. "The Communications and Social Marketing panel has emphasised the
importance of (a) using standardised messages and appropriate media and (b) focusing
communication efforts on the specific information requirements of target audiences. It has
reminded us that short-term, highly intensive efforts may be appropriate in some
situations, but only if they are part of a longer term strategy for programme
implementation. It has also called to our attention the fact that the ongoing
communication activities in ORT in developing countries are transforming the health sector
from one based exclusively on the extension of government services to one that makes use
of multiple channels. The Distribution and Logistics Panel has reminded us that government and private
sectors must work hand in hand to develop a uniform formulation and packet label and to
estimate packet needs. Local production may be relatively simple, but adequate
distribution of packets throughout the health care system requires careful planning and
monitoring of supplies. We have been rightly advised by the Panel on Health Personnel Training that
training on ORT for all health workers must include sufficient "hands-on"
experience to give the worker confidence that he or she can practise ORT and can apply
this technique even in environments where it has not been well accepted. Also, mothers can
and must be taught to prepare and administer ORT solutions in the home, but we must
remember that this task is not easy. Experience shows that mothers do not mix and give
salt and sugar solutions correctly unless they receive repeated reinforcement and
training. The Supervision and Monitoring Panel has pointed out that proper monitoring is
possible only if we determine precisely what items we want to monitor and how and when we
wish to monitor them. Unfortunately for the supervisor, such monitoring is often an
unpleasant and difficult task for which he is frequently inadequately trained and often
poorly motivated. It must become a task in which he is both competent and comfortable if
ORT use is to be effective. Innovative ways must be found to encourage and perhaps
decentralise supervision to make it effective. The Evaluation and Cost Panel concluded that obtaining data on the use of both
ORS and ORT is difficult but important. Novel approaches to measuring programme impact
need to be developed, as well as ways of measuring effective ORT use. Measuring the cost
and cost-effectiveness of ORT is important to determine optimal strategies for ORT
delivery and to convince health administrators of the economic and social benefits of this
intervention. And finally, the Panel concerned with Integrating ORT with Other Health Activities counselled
that an integrated programme can only be as strong as its individual parts. These parts
must be selected according to the public health problems of the country and the
feasibility and cost of interventions to combat them. International and bilateral agencies
must recognise that countries themselves need to make the difficult decision as to which
programmes should be given priority; support may then be given to countries to strengthen
their capabilities to undertake those programmes effectively."
|
ORT facts
- Between 1982 and 1985, the number of countries with national diarrhoeal disease control
programmes doubled.
- Access to oral rehydration salts (ORS) increased from 6 per cent in 1982 to 33 per cent
in 1985.
- Annual ORS production increased from 50 million packets in 1981 to nearly 250 million
packets in 1985
|
|
DDOnline Dialogue
on Diarrhoea Online Issue 24 March 1986 5 Page 6 7
| Channels for promoting ORT |
The traditional healer
Wilbur Hoff discusses a project in Swaziland which
recognises the importance of traditional healers in the community, and their potential for
promoting better health services. Traditional healers and modern health personnel in Swaziland are being encouraged to
work together to prevent and control diarrhoea and other children's diseases. The Ministry
of Health has organised regional training workshops for traditional healers, clinic nurses
and health inspectors. A recent evaluation of the project* showed that these training
workshops have increased traditional healers' knowledge about how to recognise, treat and
prevent childhood diseases such as diarrhoea, measles, whooping cough, tetanus,
malnutrition, diphtheria and malaria. Three important changes in attitudes and practices
were reported: Changes in treatment practices Traditional healers increased their understanding of dehydration and the treatment and
prevention of diarrhoea. Many of them accepted and used oral rehydration salts even though
they also continued to give traditional medicines (timbita) to treat diarrhoea. Both
nurses and healers reported that many healers had become aware of the harmful effects of
strong purges and enemas, which are traditionally used to treat diarrhoea, and were
beginning to discontinue their use. Co-operation between nurses and traditional healers
|
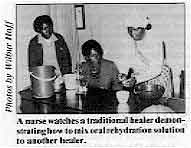
A nurse watches a traditional healer demonstrating how to mix
oral rehydration solution to another healer.
Changes in attitudes, increased communication and increased numbers of referrals to
clinics, particularly of children with severe cases of diarrhoea, were all evidence of
improved co-operation between the nurses and healers who had attended the workshops.
|
|
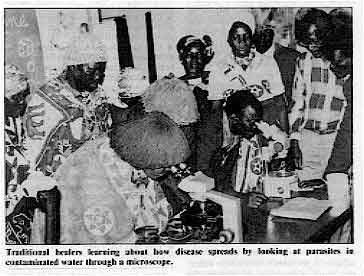
Traditional healers learning about how disease spreads by
looking at parasites in contaminated water through a microscope.
Most healers and nurses were very enthusiastic about pooling their knowledge and
resources to improve patient care, and increasing the dialogue about diagnosis, treatment
and follow-up techniques. The changed attitudes of nurses encouraged referrals to clinics.
Many healers said they were much more willing to send patients to clinics when they knew
that the nurses were interested in co-operating with them.
|
 |
Health education Traditional healers who attended the workshops had an increased awareness of the
importance of good nutrition, use of latrines, domestic and personal hygiene, and safe
water in preventing disease. Healers began to display health education materials on the
walls of their traditional clinics, and were giving preventive health advice to mothers
and other patients. In some cases the healers who had attended the workshops were
practising better health habits than those who had not: a high proportion of them had
constructed latrines and placed wash basins in their clinics. Conclusion Considering the important status and strong influence of most traditional healers among
their own people, their role in providing sound health care should not be underestimated.
In countries where health needs are great and health resources are scarce, traditional
practitioners can play a significant role in promoting self-reliance in health in rural
communities. This example from Swaziland shows what can be achieved when both the
traditional and modern health sectors agree to work together towards common goals.
Dr. Wilbur Hoff, 2230 Stuart Street, Berkeley, California 94705, USA (formerly
Health Educator for the USAID-funded Water-borne Disease Control Project in Swaziland
1983-1985.) *Co-operation between traditional healers and modern health personnel in the
control of childhood diseases in Swaziland: first phase evaluation of a pilot project.
Ministry of Health, Swaziland, January 1985.
|
|
DDOnline Dialogue
on Diarrhoea Online Issue 24 March 1986 6 Page 7 8
| Channels for promoting ORT |
The community pharmacist Professor D'Arcy describes how the pharmacist can play
an important part in the provision of oral rehydration therapy (ORT) in the community. The role of the community pharmacist in primary health care (PHC) is currently a topic
of joint discussion between WHO and the Federation Internationale Pharmaceutique (FIP),
which represents some 700,000 pharmacists in over 65 countries throughout the developed
and developing world. Because diarrhoeal disease is such a priority for concerted attack
in PHC, these discussions have focussed particularly on determining the precise role of
the community pharmacist in the prevention and treatment of this wasteful and unnecessary
disease. The pharmacist in developed countries In most developed countries the community pharmacist has long been accepted as an
integral member of the community health care team. Pharmacists, by virtue of their
graduate training and their professional responsibility have, traditionally, high
credibility with the public as dispensers of prescribed medicines, providers of
self-medication remedies, and as advisors on health care matters. Their current training,
with an emphasis on pharmacology, therapeutics and clinical pharmacy practice, well equips
them to give advice on common ailments such as diarrhoeal diseases. Commercial orientation In most developing countries, however, pharmacies are mainly situated in urban areas
where they can remain commercially viable; in some countries they tend to be rather too
commercially orientated, especially where the absence or non-enforcement of drug laws
effectively creates a non-restrictive market for medicines. It is in such an environment
that unnecessary or unsuitable sales of antibiotics and antibacterials are rampant.
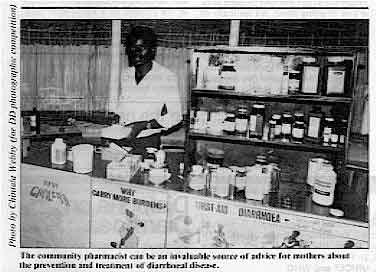 |
The community pharmacist can be an invaluable source of advice
for mothers about the prevention and treatment of diarrhoeal disease. In an increasing number of developing countries, there is a growing professionalism in
community pharmacy practice and this is the area in which a contribution towards PHC in
general, and prevention and treatment of diarrhoeal diseases in particular, can be
encouraged and developed.
|
Nigeria, Tunisia and Zimbabwe are outstanding examples of countries where pharmacists,
the government, and WHO/UNICEF have combined together in a programme to make the community
pharmacy the health education centre, especially regarding giving mothers advice in using
ORT to treat diarrhoea in children. This advice can be accompanied by simple instruction
about using the correct volume of suitable water to mix up the oral rehydration salts. The
pharmacist can also do much to convince the mother that such treatment is far better than
less effective antidiarrhoeals and potentially harmful antibiotics, by emphasising the
sale or supply of WHO-formula ORT sachets. Problems to overcome One major problem is that community pharmacies often cannot be commercially viable in
areas of sparse population; another is that many mothers still insist on purchasing
expensive (and unsuitable) antibiotics and antibacterials to treat their children. Health
education and the good advice of pharmacists will solve the latter problem in time; but
the first problem will be rather more difficult to overcome, since it involves inescapable
economic factors. Government pharmacies are a possibility, and these work well in the
Sudan, for example. Another possibility is the involvement of pharmacists in small
district hospitals, which could evolve a manufacturing and distributive role for oral
rehydration salts in rural areas. When the annual FIP Congress meets in Helsinki in September of this year, a Discussion
Forum on "Treatment and Prevention of Diarrhoeal Disease: Pharmaceutical
Involvement?" will form one of the major events of the meeting. This will do much to
formulate plans for future action and will mark the commencement of an official FIP policy
of world-wide collaboration of pharmacists in helping to combat diarrhoeal disease. Professor P. F. D'Arcy, Department of Pharmacy, The Queen's University of Belfast,
Medical Biology Centre, Lisburn Road, Belfast BT9 7BL, Northern Ireland.
|
|
DDOnline Dialogue
on Diarrhoea Online Issue 24 March 1986 7 Page 8
Creating confidence in ORS ORS is a life saver and appears to be the cheapest and simplest treatment for cases of
diarrhoea, especially those accompanied by dehydration. However, it is not an easy task to
convince our village mothers that it is a safe and effective remedy for diarrhoea. How can
a health worker convince these mothers? At our rural health centre we tried this method
and it worked effectively to some extent, though we still have a long way to go. When a
mother is sick with diarrhoea, we show her how to prepare salt/sugar solution or we give
her a packet of prepared ORS. We then tell her to drink it, ask her to stay with us for 30
minutes or so and then ask her how she feels. The mother tells us that she is feeling
stronger than when she came in for treatment. At this point we tell her how she came to
feel stronger. When she visits us again during one of her children's clinic sessions we
ask her to tell the other mothers about ORS and her experience with it. When a village
mother is given this opportunity of explaining to other mothers, they listen attentively
and have more confidence in ORS than if the explaining is done by a health worker. Pius C. Mweene, Clinical Officer, Health Centre, Mhala, Choma, Zambia.
Unnecessary i.v. therapy I recently left Iran after working there for five years in the Ministry of Health. Most
of the deaths in rural areas of Iran in the summer in infants and children are due to
dehydration caused by diarrhoea. In Iran intravenous fluid therapy is still commonly used
in the management of dehydration by general medical practitioners. Most doctors prescribe
i.v. fluids unnecessarily. Even for mild vomiting and diarrhoea, patients now expect
doctors to use i.v. therapy. This is often very harmful to the patient. Another problem is
that questionable proportions are used in i.v. fluid. Doctors never impress upon the
parents about the efficacy of oral rehydration therapy. If all GPs were to convince
parents in a proper manner, I am sure they would listen to them. It is often difficult to
persuade mothers to sit with a sick child and give oral rehydration solution for a long
period of time. The Ministry of Health has recently started training classes for health workers about
ORT, particularly in rural areas. The main problem is still to convince doctors and
hospital staff; unless doctors impress upon the people the importance of ORT, they will
never listen to health workers. Doctors should be encouraged to limit i.v. fluids and to
use ORT in all cases of mild to moderate diarrhoea. Dr. J. P. Reddy, Sri Sathya Sai Clinic & Pathological Laboratory, Near Head
Office, Nalgonda - 508 001, India.
Blindness and diarrhoea We have been running a programme for the prevention of blindness in children in India
for nearly five years. When the programme was initially launched it was thought that most
cases of corneal blindness in children followed xerophthalmia resulting from Vitamin A
deficiency and general malnutrition. Any child showing signs of xerophthalmia like night
blindness or Bitot's spots was suspected to be at risk of developing corneal ulcers or
keratomalacia. Similarly any child who was markedly underweight for its age was also
thought to be at risk of going blind. An epidemic of measles sweeping through a poor
community was also expected to leave a few children blind. All these children were given
megadoses of Vitamin A for protecting their eyes. In addition to this, each child under
the age of five years was given a six monthly prophylactic dose of 200,000 units of
Vitamin A. It was expected that with all this, childhood corneal blindness related to
Vitamin A deficiency would be totally eradicated. However, it was observed that sometimes children who were normal, without eye signs of
xerophthalmia and well nourished, would be admitted to hospital, dehydrated from
diarrhoea. Such children tend to keep their eyes partially closed and when the eyes are
opened it is found that the cornea has become soft, translucent, white and collapsed.
(Forced opening of the eyes may damage them.) Vitamin A absorption, even during diarrhoea,
has been found to be good. In some countries carrot soup has been used to prevent
dehydration and one wonders if this would be a good method to prevent post-diarrhoeal
blindness. Dr. J. V. Bhatt, Programme Director, Programme for the Prevention of Blinding
Malnutrition in Hospital, Royal Commonwealth Society for the Blind, Bombay 33, India.
DD21 update: vitamin A DD21 included a piece on diarrhoea and blindness which
featured a WHO treatment chart recommending the use of water-soluble vitamin A, given by
intramuscular injection, to prevent and treat xerophthalmia. Several readers have written
to DD to say that vitamin A in this form is not available in their area. We have been
informed by Dr. DeMaeyer of WHO that this preparation, produced solely by
Hoffman-La-Roche, is currently only available in Colombia and Switzerland, under the name
of "Water miscible AROVIT". It should be available in India from June 1986, and
Hoffman-La-Roche hope to register the product on a world-wide basis, starting in countries
such as Brazil, Pakistan and Bangladesh, although this may take some considerable time. Editors' note: Those who cannot obtain this product, should use oily vitamin A,
given by mouth, which produces very effective blood-levels within hours.
|
In the next issue...
DD 25 will
focus on drug therapy for of the most recent findings about |

Scientific editors Dr Katherine Elliott and Dr William Cutting
Editor Kathy Attawell
Editorial assistant Maria Spyrou Editorial advisory group
Professor David Candy (UK)
Professor Richard Feachem (UK)
Dr Michael Gracey (Australia)
Dr Norbert Hirschhom (USA)
Professor Leonardo Mata (Costa Rica)
Dr Majibur Rahaman (Bangladesh)
Dr Jon Rohde (USA)
Ms E O Sullesta (Philippines)
Professor Andrew Tomkins (UK)
Dr Paul Vesin (France)
Dr M K Were (Kenya) With support from AID (USA), UNICEFand WHO
|
Issue no. 24 March 1986
Page Navigation
This edition of Dialogue on Diarrhoea Online is produced by Rehydration Project. Dialogue on Diarrhoea was published four times a year in English, Chinese, French, Portuguese, Spanish, Tamil,
English/Urdu and Vietnamese and reached more than a quarter of a million readers worldwide. The English edition of Dialogue on Diarrhoea was produced and distributed by Healthlink Worldwide. Healthlink Worldwide is committed to strengthening primary health care and
community-based rehabilitation in the South by maximising the use and impact
of information, providing training and resources, and actively supporting
the capacity building of partner organisations. - ISSN 0950-0235 Reproducing articles
Healthlink Worldwide encourages the reproduction of
articles in this newsletter for non-profit making and educational uses. Please
clearly credit Healthlink Worldwide as the source and, if possible, send us a copy of any uses made of the material.
|
updated: 23 April, 2014
updated: 23 April, 2014
|






